ECR 2020 / C-06620
Breast enlargement: a challenging sign.
Congress:
ECR 2020
Poster Number:
C-06620
Type:
Educational Exhibit
Keywords:
Performed at one institution, Not applicable, Pathology, Neoplasia, Diagnostic procedure, Biopsy, Ultrasound, MR, Mammography, Breast
Authors:
R. M. Lorente Ramos, F. J. Azpeitia Armán, C. Oliva Fonte, J. M. García Gómez, J. M. Lopez-Arcas Callejas, F. Fernández Alarza; Madrid/ES
DOI:
10.26044/ecr2020/C-06620

Fig. 1:
Normal variants

Fig. 2:
Gynecomastia

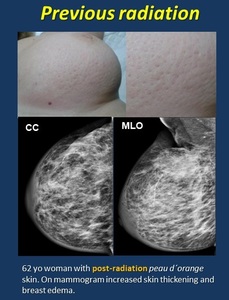
Fig. 3:
Previous radiation

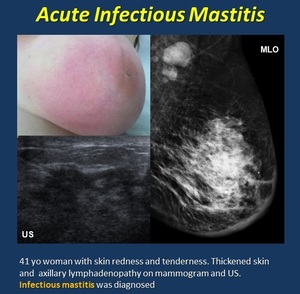
Fig. 4:
Mastitis
.")
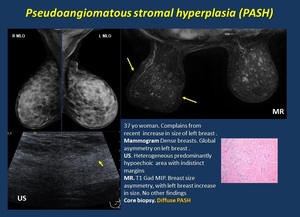
Fig. 5:
Pseudoangiomatous stromal hyperplasia (PASH).
.")
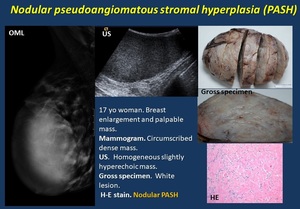
Fig. 6:
Nodular pseudoangiomatous stromal hyperplasia (PASH).

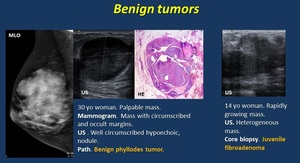
Fig. 7:
Benign tumors

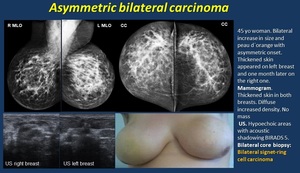
Fig. 8:
Asymmetric bilateral carcinoma

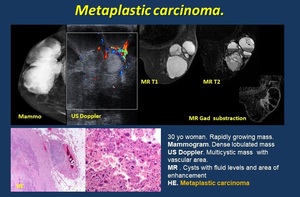
Fig. 9:
Metaplastic carcinoma

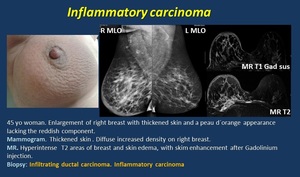
Fig. 10:
Inflammatory carcinoma

Table 2:
Diagnostic criteria for inflammatory carcinoma.

Fig. 11:
Breast primary lymphoma

Fig. 12:
Angiosarcoma

Fig. 13:
Metastases

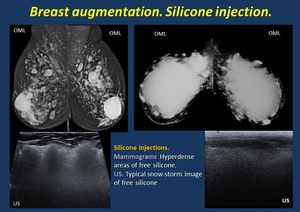
Fig. 14:
Silicone injection

Fig. 15:
Hyaluronic acid

Fig. 16:
Periprosthesis fluid

Fig. 17:
Prosthesis rupture

Fig. 18:
Congestive heart failure

Fig. 19:
SVC Syndrome

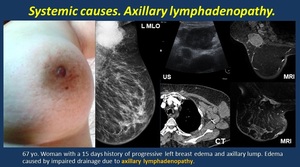
Fig. 20:
Axillary lynphadenopathy

Fig. 21:
Dermal lesions

Fig. 22:
Pectoralis muscle lipoma

Fig. 23:
Pectoralis muscle liposarcoma

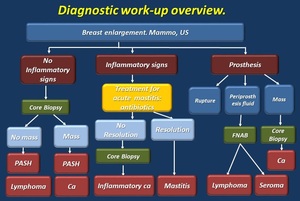
Fig. 24:
Diagnostic work-up

Table 3