ECR 2020 / C-08529
Contemporary multimodality imaging of pericardial diseases: a guide for the radiologist
Congress:
ECR 2020
Poster Number:
C-08529
Type:
Educational Exhibit
Keywords:
Cardiac, CT, MR, Diagnostic procedure, Inflammation, Not applicable
Authors:
P. Simkus1, A. Banišauskaitė1, J. Noreikaite2, V. Buroviené1, M. Gutierrez3, A. Jankauskas1, M. Arzanauskaite2; 1Kaunas/LT, 2Liverpool/UK, 3barcelona/ES
DOI:
10.26044/ecr2020/C-08529

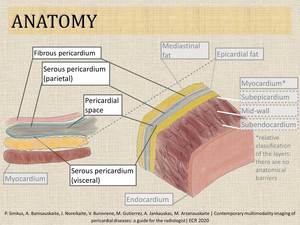
Fig. 1:
Anatomy of pericardium.

Fig. 2:
Normal pericardium.

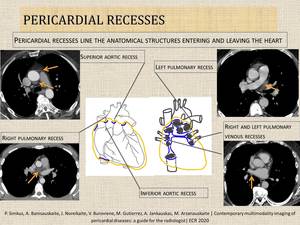
Fig. 3:
Pericardial recesses.

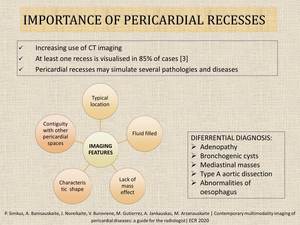
Fig. 4:
Importance of pericardial recesses.

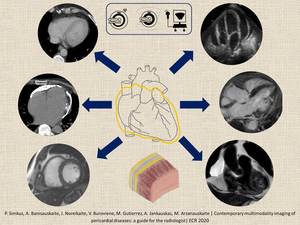
Fig. 5:
Contemporary multimodality imaging of pericardial diseases

Table 1:
Advantages and limitations of imaging modalities [4].

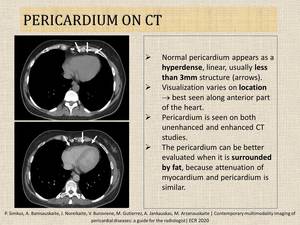
Fig. 6:
Normal appearance of pericardium on CT.

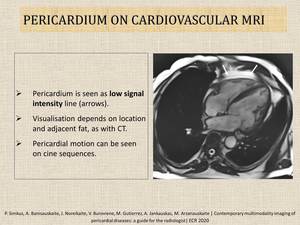
Fig. 7:
Normal appearance of pericardium on cardiovascular MRI.

Fig. 9:
Pericardial cyst.

Table 2:
Aetiology of pericardial effusions.

Fig. 10:
Hydropneumopericardium.

Fig. 11:
Pericardial haematoma.

Fig. 12:
Acute pericarditis with pericardial effusion.

Fig. 13:
Peri-infarct pericarditis.

Fig. 14:
Constrictive pericarditis.

Table 3:
Main pericardial tumours.

Fig. 16:
Metastasis in the pericardium.