Imaging the PPF
CT:
- The fat filled is hypodense on CT- Loss of this normal fat signal is an important indicator of infiltration by pathological process
- CT provides excellent bony detail to assess for bone erosion and ensure symmetric calibre of multiple foramen
MRI:
- T1-weighted imaging (T1WI) is most beneficial for initial assessement- demonstrates normal symmetric high fat signal in PPF.
- Can see flow voids due to maxillary artery and mild post-gadolinium enhancement secondary to emissary veins
- Multiplanar post-gadolinium imaging best modality to assess for perineural spread (PNS)

Fig. 1: CT of PPF in axial soft tissue (left) and axial (middle) and sagittal (right) bone windows. Note the normal fat density of the fossa on soft tissue windows
Anatomy:
The pterygopalatine fossa (PPF) is located between the posterior maxillary sinus wall and pterygoid process of sphenoid bone.
It has extensive communications throughout the head and neck (H&N) which can facilitate the dissemination of pathologies throughout the H&N.
Boundries:
Anterior: Maxillary sinus
Posterior: Pterygoid process
Inferior: Palatine bone
Superior: Inferior orbital fissure
Medial: Perpendicular plate of palatine bone
Lateral: Pterygomaxillary fissure
Contents:
Maxillary division of trigeminal nerve (V2)
Pterygoid ganglion
Terminal 1/3rd of the maxillary artery
Communications
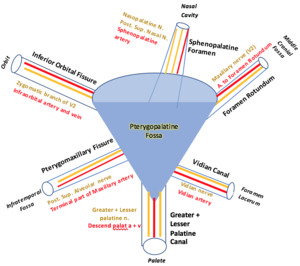
Fig. 2: Schematic diagram of the PPF with it's communications and their contents.
Foramen Rotundum
- Extends from middle cranial fossa to PPF (posterior aspect)
- Traverses through the sphenoid bone
Contents
- V2 nerve
- Artery to foramen rotundum and emissary veins
Imaging
- Best seen on coronal images- superolateral to Vidian canal in sphenoid bone
- Located at same axial level as the inferior orbital fissure

Fig. 3: Axial (left) and coronal CT images of foramen rotundum. Note the superolateral relationship to vidian canal on coronal image.
Inferior orbital fissure:
- Extends from anterior PPF to orbit (opens into posterolateral aspect of orbital floor)
- Traverses in fissure between greater wing of sphenoid superiorly and maxilla inferiorly
- Joins with Pterygomaxillary fissure medially
Contents:
- Zygomatic branch of V2
- Infraorbital nerves and vessels
- Branches of inferior ophthalmic vein
- Orbital ganglionic branches
Imaging
- Posterior portion of fissure best appreciated on coronal imaging
- Located at the same axial level as foramen rotundum

Fig. 4: Axial CT of inferior orbital fissure
Pterygomaxillary fissure
- Connects PPF to masticator and infratemporal space
- Long triangular fissure formed from divergence of maxilla from pterygoid process. Located on lateral aspect of PPF.
Contents
- Superior alveolar nerve
- Terminal branches of maxillary artery
Imaging:
- Wide fissure readily identifiable on axial imaging
- Primary soft tissue sarcomas or odontogenic infections of masticator space can directly extend into the PPF via the Pterygomaxillary fissure

Fig. 5: Axial CT of pterygomaxillary fissure
Sphenopalatine foramen
- Connects PPF to superior meatus of the nasal cavity
- Originates from the medial aspect of PPF at the palatine and sphenoid bone junction
Contents:
- Nasopalatine and posterior superior nasal nerves
- Sphenopalatine artery and vein
Imaging:
- At the same axial levels as the Vidian canal
- Juvenile Nasopharyngeal Angiofibroma is typically centred on the sphenopalatine foramen

Fig. 6: Axial CT of sphenopalatine foramen
Vidian Canal
- Connects middle cranial fossa (just anterior to foramen Lacerum) to PPF
- Enters the posterior aspect of PPF
Contents:
Imaging:
- Inferomedial to foramen rotundum- best appreciated on coronal
- Axial- thin foramen originating anterior to foramen Lacerum

Fig. 7: Axial (left) and coronal (right) CT of vidian canal. Note the inferomedial relationship to foramen rotundum on coronal image.
Greater palatine canal
- Connects PPF to palate
- Originates from inferior aspect of PPF
- This foramen gives rise to a small accessory canal- lesser palatine canal. It opens in the palate posterior to the greater palatine canal
Contents
- Greater + lesser palatine nerves
- Descending palatine artery

Fig. 8: Axial CT of greater palatine canal.
Pathologies
Key imaging features of PPF infiltration by pathology includes
- Obliteration of normal fat signal/density in PPF
- Widening of PPF or its canals
- Bony erosions of PPF walls
The extensive communications outlined above can act as a highway to disseminate pathologies throughout the H&N spaces.
Lesions can spread into the PPF via direct extension or perineural spread (PNS).
PNS
- PNS is direct neoplastic extension from primary tumour along the tissues of the nerve sheath
- PNS drastically changes prognosis with a 3-fold increase in local recurrence and approximately 30% decrease in 5 year survival rate
- V2 , V3 and facial nerves are most commonly implicated
- PNS tends to occur in a retrograde fashion
Imaging features of PNS:
- Enhancement of nerve
- Soft tissue thickening of the nerve
- Increased calibre of its foramen
- Best appreciated on post-contrast fat saturated T1WI
Direct extension into PPF
Juvenile Nasopharyngeal Angiofibroma
- Benign, locally invasive vascular tumour typically originating from the sphenopalatine foramen. Occurs almost exclusively in males aged 10-20 years old. Clinical presentation is recurrent epistaxis with nasal obstruction.
- Majoity (90%) extend into the PPF via sphenopalatine foramen
Imaging:
- Avidly enhancing vascular mass
- CT- avidly enhancing mass. Bone remodelling/destruction with widening of sphenopalatine foramen
- MRI- post-contrast fat saturated T1WI is best to delineate lesion and evaluate degree of extension
- Direct angiography (usually with embolization) is performed pre-operatively. Usually supplied by internal maxillary branch.

Fig. 9: Juvenile Nasopharyngeal Angiofibroma- 19 year old male with nasal obstruction and epistaxis
Axial and sagittal post-contrast CT (top) demonstrating avidly enhancing mass centered on, and widening, the left sphenopalatine foramen. The vascular mass extends posteriorly into the left PPF.
Direct angiography (bottom left) demonstrates strong vascular blush from distal internal maxillary artery with successful embolisation (bottom left) prior to surgical excision.
Nasopharyngeal Carcinoma
- Mucosal tumour of the nasopharynx typically centered on Fossa of Rosenmüller
- Common in Asia, 3:1 male predilection, aged 40-60.
- Strong association with EBV infection
- Presentation is typically late with nodal metastasis present in 90% at diagnosis.
- Locally advanced tumours can extend superiorly and, via bony destruction, infiltrate directly into PPF

Fig. 11: 77 year old presented with left V2 palsy
Axial CT with soft tissue windows (top left) demonstrates infiltrative soft tissue involving the left PPF
Axial (top right) and coronal (bottom right) post-contrast T1WI demonstrate infiltration of left PPF with perineural spread along foramen rotundum (straight arrow) with extensive involvement of Meckel's cave (curved arrow).
Axial CT in bone windows (bottom left) demonstrates widening of vidian canal in keeping with PNS.
Nasopharyngeal carcinoma confirmed on histopathology.

Fig. 10: 76 year old male. Presented to ED with confusion, Incidental large nasopharyngeal mass identified on CT brain. History revealed 2 year history of nasal obstruction, discharge and headaches.
Post-contrast T1WI with fat saturation images identify large infiltrating nasopharyngeal mass (straight arrow).
Widening of left foramen rotundum with infiltrating PNS of tumour along the foramen (curved arrow).
PNS also identified along inferior orbital fissure (dotted arrow)
Diagnosis of nasopharyngeal carcinoma confirmed on histopathology.
Masticator space sarcoma
- Mesenchymal tumours such as rhabdomyosarcoma and fibrosarcoma are most common primary tumours of the masticator space.
- If these lesions infiltrate medially they can extend to the PPF via the Pterygomaxillary fissure.
Perineural Spread (PNS)
Adenoid Cystic Carcinoma (ACC)
- ACC is a rare slow-growing adenocarcinoma of glandular origin- most commonly in H&N salivary glands, paranasal sinuses and nose.
- ACC has a high propensity for PNS and is seen in as much as 60% of cases.
Sinonasal SCC
- Sinonasal (typically nasal cavity or maxillary sinus) is a relatively rare location for SCC. Increasingly recognised association with HPV
- Thses lesions are characterised by aggressive growth and bony destruction often eroding and extending beyond the sinus walls.
- In nasal cavity and maxillary sinus, these lesions can directly extend into PPF via bony destruction or through PNS via sphenopalatine foramen.

Fig. 14: 69 year old male. Prior right endoscopic maxillectomy for sinonasal SCC- follow up MRI 6 months later.
CT demonstrates bony destruction of the posterior/lateral wall of the right maxillary sinus (straight red arrow)
Axial T2 (top middle) shows soft tissue along lateral maxillary wall (dotted red arrow) and loss of normal signal in right PPF (curved red arrow)
Axial T2 (top right) shows PNS of soft tissue along inferior orbital fissure.
Axial T1WI post-contrast (bottom images) show enhancement along vidian canal (dotted blue arrow) and foramen rotundum (curved blue arrow) in keeping with PNS
Metastasis
- Metastasis to the H&N are rare but can be the first presentation of an unknown primary
- As shown in the accompanying case- metastasis to the orbit can infiltrate posteriorly along the inferior orbital fissure into the PPF. Potential primary sources include breast, lung, prostate, GO, kidney and skin
- Thyroid malignancies have been shown to metastasise to the sinuses

Fig. 12: 55 year old woman with history of breast cancer presented with left-sided diplopia, restricted eye movements and ptosis.
T1 (top left) T1 post contrast axial (top right) and coronal (bottom)
Axial T1WI pre-contrast demonstrates loss of normal fat signal in PPF (Dotted arrow).
Post contrast T1WI demonstrates infiltrative lesion involving the left orbital apex which extension posteriorly via inferior orbital fissure (straight arrow) into the PPF. There is evidence of PNS along foramen rotundum into Meckel's cave (curved arrow).
Non-neoplastic
Fungal Sinusitis
- Invasive fungal sinusitis is seen in immunocompromised patients and uncontrolled diabetics. It is a progressive process and can present as life-threatening disease. It can infiltrate into the PPF and extend on into the middle cranial fossa via direct extension or PNS by foramen rotundum. Disease involving the PPF requires urgent surgical input.
Granulomatosis with polyangiitis
- GPA (Formerly Wegener’s) is a multisystem necrotising, non-caseating granulomatous c-ANCA positive vasculitis. The majority (72-100%) of patients with GPA have upper respiratory tract involvement with manifestations such as sinusitis, mastoiditis and otitis.
- Direct granulomatous extension and PNS are potential modes of infiltration for sinonasal GPA.

Fig. 13: 42 year old male with symptoms of chronic sinusitis.
Axial T1WI pre (left) and post (right) contrast.
Mucosal opacification of the right maxillary sinus (straight arrow).
Loss of normal T1 fat signal in right PFF (dotted arrow).
Post-contrast demonstrates widening and infiltrative enhancement along foramen rotundum (curved arrow)
Systematic Approach
- Firstly the PPF should be included as a “review-area” for cross-sectional imaging of the brain to ensure it contains the normal fat signal/density as described above.
- When a lesion in the PPF is encountered it is crucial all the communications are individually assessed to ensure accurate description of the extent of infiltration. By using a list of these communications as part of PPF lesion assessment it can help to ensure subtle but clinical important extension is not missed.
- Middle cranial fossa-Foramen rotundum and Vidian Canal
- Nasal cavity-Sphenopalatine foramen
- Infratemporal fossa-Sphenopalatine foramen
- Orbit-Inferior orbital fissure
- Palate-Greater+lesser palatine canals


 and axial (middle) and sagittal (right) bone windows. Note the normal fat density of the fossa on soft tissue windows")
 and coronal CT images of foramen rotundum. Note the superolateral relationship to vidian canal on coronal image.")



 and coronal (right) CT of vidian canal. Note the inferomedial relationship to foramen rotundum on coronal image.")

 demonstrating avidly enhancing mass centered on, and widening, the left sphenopalatine foramen. The vascular mass extends posteriorly into the left PPF.
Direct angiography (bottom left) demonstrates strong vascular blush from distal internal maxillary artery with successful embolisation (bottom left) prior to surgical excision.")
.
Widening of left foramen rotundum with infiltrating PNS of tumour along the foramen (curved arrow).
PNS also identified along inferior orbital fissure (dotted arrow)
Diagnosis of nasopharyngeal carcinoma confirmed on histopathology.")
 demonstrates infiltrative soft tissue involving the left PPF
Axial (top right) and coronal (bottom right) post-contrast T1WI demonstrate infiltration of left PPF with perineural spread along foramen rotundum (straight arrow) with extensive involvement of Meckel's cave (curved arrow).
Axial CT in bone windows (bottom left) demonstrates widening of vidian canal in keeping with PNS.
Nasopharyngeal carcinoma confirmed on histopathology.")
 T1 post contrast axial (top right) and coronal (bottom)
Axial T1WI pre-contrast demonstrates loss of normal fat signal in PPF (Dotted arrow).
Post contrast T1WI demonstrates infiltrative lesion involving the left orbital apex which extension posteriorly via inferior orbital fissure (straight arrow) into the PPF. There is evidence of PNS along foramen rotundum into Meckel's cave (curved arrow).")
 and post (right) contrast.
Mucosal opacification of the right maxillary sinus (straight arrow).
Loss of normal T1 fat signal in right PFF (dotted arrow).
Post-contrast demonstrates widening and infiltrative enhancement along foramen rotundum (curved arrow)")

Axial T2 (top middle) shows soft tissue along lateral maxillary wall (dotted red arrow) and loss of normal signal in right PPF (curved red arrow)
Axial T2 (top right) shows PNS of soft tissue along inferior orbital fissure.
Axial T1WI post-contrast (bottom images) show enhancement along vidian canal (dotted blue arrow) and foramen rotundum (curved blue arrow) in keeping with PNS")