This paper presents the CT findings of perigraft fluid collections after RT, emphasizing the importance of the imaging investigation in diagnosing and choosing the best therapy.
We have designed a 15-year retrospective study including 93 patients who developed perigraft fluid collections after a kidney transplant. The results revealed that 31% of the patients developed hematomas, 55% lymphoceles, 10% urinomas and 4% abscesses ( Fig. 4 ). Comparable to published data3, our study revealed that lymphoceles are the most frequent perigraft collections, having the best prognosis.
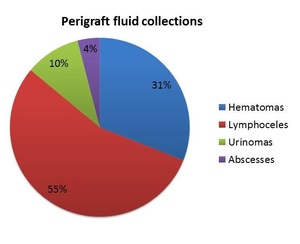
Fig. 4: The frequencies of perirenal graft fluid collection in our group of patients
References: Cristache Ioan Andrei
The patients were evaluated with enhanced and unenhanced multislice CT (MSCT).
Computed tomography (CT) tehnique
Unenhanced CT - provides general overview of these fluid collections.
Enhanced CT - offers a more specific image upon the lesions in patients with normal renal function:
- Cortico-medullary phase (late arterial phase): 35-40 seconds post injection of contrast material (CM)
- Nephrographic phase (venous phase): 80-90 seconds after the beginning of the CM injection;
- Excretory phase (EP): between 7 minutes to a couple of hours after the CM injection.
CT FINDINGS
1. Perigraft hematomas
In our patients, perigraft hematomas were found early after surgery, both in the perirenal and subcapsular space.
CT. Regarding the CT aspects:
- in acute phases they are spontaneously hyperdense ( Fig. 5 ) .
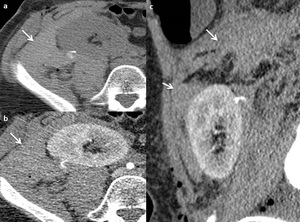
Fig. 5: Perirenal graft hematoma. Unenhanced (a) and enhanced CT in cortico-medullary phase (b,c). Large perirenal high attenuating nonenhancing collection (arrow).
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania
- in late phases the density drops progressively ( Fig. 6 ).
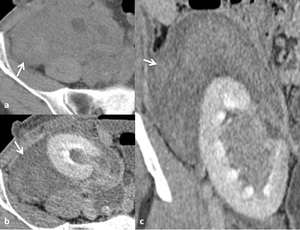
Fig. 6: Perirenal graft hematoma. Unenhanced (a) and enhanced CT in excretory phase (b,c): Large perirenal inhomogeneous hyperdense nonenhancing collection (arrow) with different degrees of attenuation.
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania
- active bleeding is shown as extravasation of contrast into perirenal space ( Fig. 7 ).
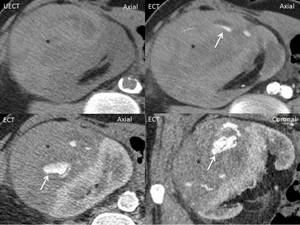
Fig. 7: Pererenal graft hematoma. Unenhanced (a) and enhanced CT in cortico-medullary (b) and nephrogenic phase (c,d). Large perirenal high attenuating nonenhancing collection (*) with active bleeding - extravasation of contrast into perirenal space (arrow).
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania
Hematomas appear as areas of high attenuation, that being the main difference between blood and the other collections.
The attenuation of blood differs depending on the moment of evaluation: when the extravascular blood is still unclotted, the measured attenuation is 30-45 HU and when the clot is already formed, it is 45-70 HU. Near the site of hemorrhage the hematoma has the highest attenuation – sentinel clot sign, while unclotted blood have lower attenuation and is located further from the source7,8.
When seen on CT, active bleeding requires emergency in actions: embolization or surgical treatment.
Treatment: The choice between open surgery or interventional radiology depends on the location of the leak, the vascularization of the transplanted kidney and involved ureter and the presence of any complications caused by blood leak5,7,8 ( Fig. 8 ).
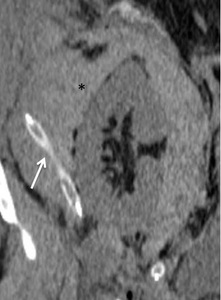
Fig. 8: Perirenal graft hematoma. Unenhanced CT showing a: perirenal high-attenuating nonenhancing collection (*) with a surgical drain included.
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania
2. Perigraft lymphoceles
Our results showed that lymphoceles are the most common collections encountered in our group of patients, after RT. They are caused by lymphatic channels damage.
CT. On CT, lymphoceles appear as fluid density collections, usually on the medial aspect of transplanted kidney, between the graft and the bladder. They usually are sharply circumscribed fluid collections with attenuation values similar to water and lower than those of recent hematomas and abscesses, without any enhancement after intravenous contrast material injection9 ( Fig. 9 ).
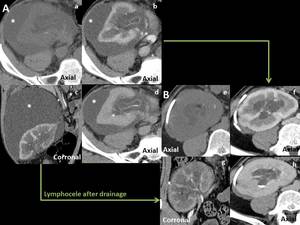
Fig. 9: Perirenal graft lymphocele. Unenhanced (a,e) and enhanced CT in cortico-medullary (b,c,f,g) and excretory phase (d,h). Perirenal graft lymphocele: A: large perirenal fluid density collection, sharply circumscribed and without any enhancement after CM injection (*). B: CT aspect of the collection after drainage.
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania
As we found in our reports, lymphoceles can get infected, acquiring the CT aspects of abscesses. ( Fig. 10 )

Fig. 10: Perirenal graft abscess: Enhanced CT in nephrogenic phase (a,b) and excretory phase (c) showing perirenal graft abscess developed after an undtreated lymphocele.
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania
Treatment: The therapeutic approach can vary, depending on the clinical status of the patient, the size, location, infection risk, loculations and recurrence risk of the collections. On one hand, small lymphoceles require only ultrasonographically monitoring. On the other hand, larger and symptomatic lymphoceles can be initially treated by percutaneous drainage or aspiration with or without instillation of sclerosing agents such as Tetracycline, but there is a high risk of recurrence ( Fig. 9 ). Laparoscopic drainage may be tried for sterile lymphoceles (laparoscopic marsupialization)6,8,9.
Fig. 9: Perirenal graft lymphocele. Unenhanced (a,e) and enhanced CT in cortico-medullary (b,c,f,g) and excretory phase (d,h). Perirenal graft lymphocele: A: large perirenal fluid density collection, sharply circumscribed and without any enhancement after CM injection (*). B: CT aspect of the collection after drainage.
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania
3. Perigraft urinomas
Urinomas are fluid collections that form because of urine leakage from the renal pelvis, ureter or ureteroneocystostomy site (secondary to necrosis of the distal ureter).
CT. Perirenal transplant urinomas appear as fluid collections on precontrast CT scan and in the early postcontrast phases; in the delayed excretory phases (obtained 5–20 minutes after contrast material injection), the urine leakage is demonstrated by increased attenuation contrast in the perinephric collection, due to a fistula in the new urinary tract ( Fig. 11 ). The CT imaging reveals urinomas as both encapsulated fluid collection and free intraperitoneal fluid1,3,4 .
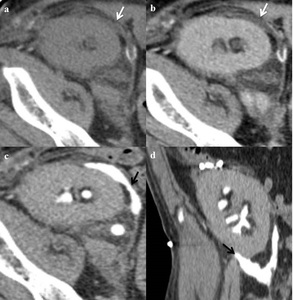
Fig. 11: Perirenal graft urinoma. Unenhanced (a) and enhanced CT in nephrogenic (b) and late excretory phases (c,d). Perirenal low attenuating collection on unenhanced examination and nephrogenic phase (white arrows) and progressively increasing attenuation on late excretory phase because of CM extravasation in the perirnenal space, demonstrating urine leakage (black arrows).
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania
Treatment: Depending on the size and position of the urinomas, they can be treated by percutaneous drainage of the collection or by adressing firstly the urinary leakage with antegrade and retrograde stenting of the ureter (with or without percutaneous drainage of the collection). Also, percutaneous nephrostomy, used to divert the urinary flow, with ureteral stent placement can treat a majority of cases. When the percutaneous approach is not possible or insufficient, subsequent surgery may be necessary. For the management of urinary leakage, surgical techniques include: anastomosis of the renal graft pelvis to the adjacent native ureter and anastomosis of the transplant ureter to the native ureter1,4,6.
4. Abscesses and infected perigraft collections
As stated also in scientific literature3, we found that abscesses are rarely found after RT.
CT. The CT scan reveals single or multiloculated low-attenuation fluid collections with thick walls of high enhancement (after injection of contrast medium) ( Fig. 12 ). Gas bubbles may be found within the abscess cavity and in the adjacent soft tissue4.
Treatment: Percutaneous drainage is the key treatment for abscesses, in association with antibiotic therapy (for sepsis control and prevention of infection spreading). In difficult cases of kidney malfunctioning or severe infection, the main treatment remains open or laparoscopic nephrectomy4,8.
5. Perigraft mixt collections
Besides the classical aspects of the perigraft fluid collections prior described, we can also find mixt collections. In our case, we encountered one case, having both CT aspects of urinoma and hematoma, an uro-hematoma ( Fig. 13 ).
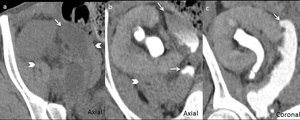
Fig. 13: Perirenal graft uro-hematoma. Unenhanced (a) and enhanced CT in late excretory phase (b,c). Inhomogeneous perigraft fluid collection with different degrees of attenuation, varying from fluid to hematic densities (arrow head), progressively filling with CM in the late excretory phase (urine leakage- arrow).
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania


 and enhanced CT in cortico-medullary phase (b,c). Large perirenal high attenuating nonenhancing collection (arrow). References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")
 and enhanced CT in excretory phase (b,c): Large perirenal inhomogeneous hyperdense nonenhancing collection (arrow) with different degrees of attenuation. References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")
 and enhanced CT in cortico-medullary (b) and nephrogenic phase (c,d). Large perirenal high attenuating nonenhancing collection (*) with active bleeding - extravasation of contrast into perirenal space (arrow). References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")
 with a surgical drain included. References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")
 and enhanced CT in cortico-medullary (b,c,f,g) and excretory phase (d,h). Perirenal graft lymphocele: A: large perirenal fluid density collection, sharply circumscribed and without any enhancement after CM injection (*). B: CT aspect of the collection after drainage. References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")
 and excretory phase (c) showing perirenal graft abscess developed after an undtreated lymphocele. References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")
 and enhanced CT in nephrogenic (b) and late excretory phases (c,d). Perirenal low attenuating collection on unenhanced examination and nephrogenic phase (white arrows) and progressively increasing attenuation on late excretory phase because of CM extravasation in the perirnenal space, demonstrating urine leakage (black arrows). References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")
 and enhanced CT in nephrogenic (b), early excretory (c) and late excretory phases (d). Large perirenal graft flluid collection with thick high enhancing walls (arrow), located lateral to the bladder (*). References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")
 and enhanced CT in late excretory phase (b,c). Inhomogeneous perigraft fluid collection with different degrees of attenuation, varying from fluid to hematic densities (arrow head), progressively filling with CM in the late excretory phase (urine leakage- arrow).
References: Radiology, Medical Imaging and Interventional Radiology of Fundeni Clinical Institute, Bucharest, Romania")