ECR 2020 / C-12476
Circle of Willis anatomical variants - disease or the norm?
Congress:
ECR 2020
Poster Number:
C-12476
Type:
Scientific Exhibit
Keywords:
Vascular, Neuroradiology brain, MR-Angiography, Computer Applications-Detection, diagnosis, Radiobiology, Developmental disease, Image verification, Prospective, Observational, Performed at one institution
Authors:
J. Sidorova, A. I. Gromov, A. Kudryavtseva, M. Starodubtseva; Moscow/RU
DOI:
10.26044/ecr2020/C-12476
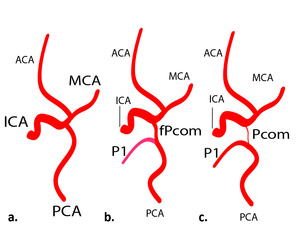
 fetal, b) transitional, c) adult.")
Fig. 3:
Scheme of cerebral arterial types reflecting of fetal circulation development...

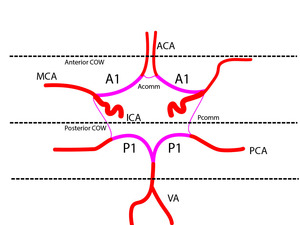
Fig. 4:
Scheme of arteries that compose the COW
. a) Standard. b) With arteries of corpus callosum from Acomm (arrow).")
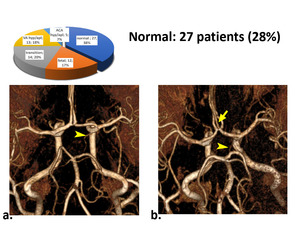
Fig. 5:
Normal cerebral circulation type, one side thin Pcomm visible (arrowheads). a)...
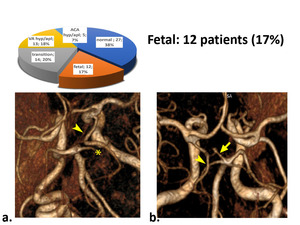
. a) Fetal type with aplasia P1, superior cerebellar artery (*). b) Fetal type with hypoplasia P1 (arrow).")
Fig. 6:
Fetal cerebral circulation type, PCA from ICA are seen (arrowheads). a) Fetal...
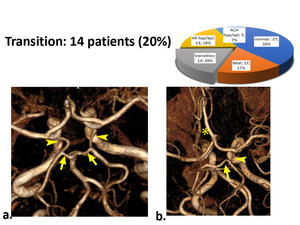
 in equal diameter with P1 (arrow). a) Bilateral transition type. b) Unilateral transition type with ACA azigos (*).")
Fig. 7:
Transitional cerebral circulation type, Pcomm are seen (arrowheads) in equal...
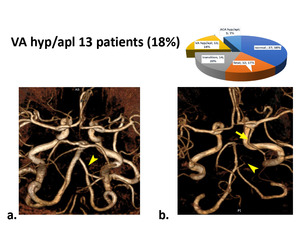
. a) Unequal diameter of VA. b) Aplasia of VA and its transition to the cerebellar artery (arrowhead), combined with the fetal type (arrow).")
Fig. 8:
Type of hypoplasia or aplasia of VA (arrowheads). a) Unequal diameter of VA. b)...
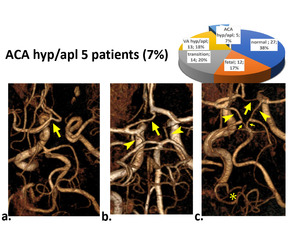
 ACA aplasia on one side and ACA bifurcation on the other side (arrow). b) Aplasia of the A1 segment of ACA (arrow), combined with the bilateral transition type (arrowhead). c) Multiple variants: Aplasia of A1 segment of ACA (arrow), bilateral fetal type (arrowheads) with P1 segment of PCA hypoplasia (arrow), VA aplasia (*).")
Fig. 9:
Type of hypoplasia or aplasia of ACA. a) ACA aplasia on one side and ACA...

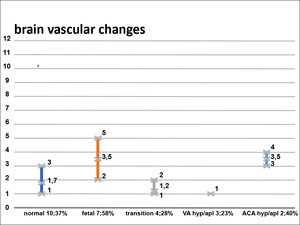
Fig. 10:
Diagram 1

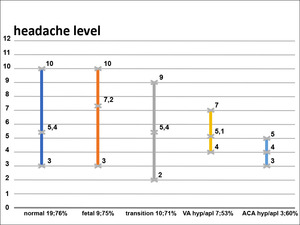
Fig. 11:
Diagram 2

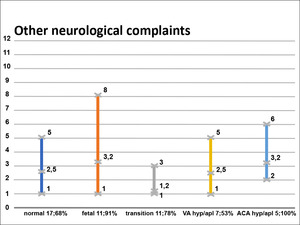
Fig. 12:
Diagram 3

Fig. 13:
Diagram 4