JUVENIL KYPHOSIS (SCHEUERMANN'S DISEASE)
Kyphosis in the thoracic spine means exaggerated kyphotic angle from the spine's normal kyphotic curve.
Kyphosis is classified as either postural or structural.
- Postural means the kyphosis is attributed to poor posture,
usually presenting a smooth curve,
which can be corrected by the patient.
- Structural kyphosis is caused by an abnormality affecting the bones,
intervertebral discs,
nerves,
ligaments,
or muscles
Posterior thoracic convexity is normally 20° to 40°.
Dorsal kyphosis over 40 ° with involvement of at least 4-5 vertebrae and kyphosis under 20° are considered pathological conditions.
The Cobb Angle Method measures the kyphotic curve in degrees using a standard full-length lateral x-ray.
Fig. 6
For kyphosis,
on lateral view,
a line is drawn along the superior end plate of the superior end vertebra and a second line drawn along the inferior end plate of the inferior end vertebra.
The angle formed by intersection of lines perpendicular to above mentioned lines is Cobb angle for kyphosis.
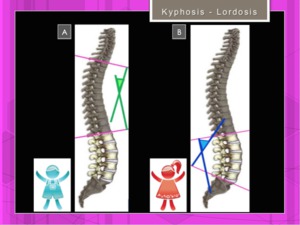
Fig. 6: Cobb angles: dorsal kyphosis (more frequent in male)(A) and lumbar lordosis (B)(more frequent in female
References: Hospital of Galdácano. Radiology
Scheuermann's disease is a thoracic or thoracolumbar hyperkyphosis due to wedged vertebrae developing during adolescence.
The true incidence of juvenile kyphosis is not known.
Its exact etiology is unknown.
Genetic factors have been described [3].
A growth disturbance of the encholdral ossification ,
with increased proteoglycan content of the matrix and diminished number of collagen fibers is observed. In the afected anterior areas of the vertebral bodies the growth process is slowed down.
It's not exactly a destruction.
Fig. 7

Fig. 7: Scheuermann Disease: Pathogenesis.Multiple factors including a growth disturbance has been described. Stop/absence of growth in the anterior areas of the wedged-shaped vertebral endplates.
References: Hospital of Galdácano. Radiology
The results is a wedge-shaped deformation of the vertebrae and an increase in kyphosis [4].
According to Sörensen [5] and Bradford [6] the diagnostic criteria for Juvenil Kyphosis (Type I) are:
- wedging of more than 5 degrees in one or more vertebrae in the thoracic or thoracolumbar region
- endplate irregularities
- disc space narrowing
- increased thoracic or thoracolumbar kyphosis
Schmorl's nodes are not pathognomonic !!!
Diagnostic criteria for Juvenil Kyphosis (Type II,
"Lumbar"):
- endplate irregularities in one or several vertebral bodies of the lumbar or thoracolumbar area
- increased sagittal diameter of vertebra bodies
- disc space narrowing
- apophyseal separation
- loss of lumbar lordosis or slight kyphosis
- Schmorl's node
( Fig. 8 ,
Fig. 9 )

Fig. 8: Scheuermann's disease: Type I and Type II.
References: Hospital of Galdácano. Radiology
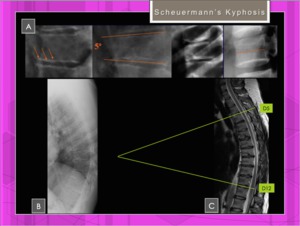
Fig. 9: Scheuermann disease type I: Features.
References: Hospital of Galdácano. Radiology
The main symptoms of Juvenile kyphosis are:
- back pain
- cosmetic disturbance with a rigid thoracic spine
Differential diagnosis between Juvenile Kyphosis (Type I) and Idiopathic Roundback:
- In the Idiopathic roundback the hyperkyphosis is harmonic also in flexion
- In the Idiopathic Roundback the hyperkyphosis corrects in extension
Imaging Studies
- Plain lateral and posteroanterior radiographs of the whole spine with the patient in standing position.
- MRI of the whole spine.
the imaging modality of choice
Treatment:
- Exercise,
bracing and casting in most of patients
- Surgery indications:
- neurological compromise
- curves >75 degrees
- progressive curves
- painful disease
SCOLIOSIS
Definition: Scoliosis is defined as the presence of one or more lateral curves of the vertebral column in the coronal plane with a Cobb angle of 10° or more,
although abnormal curves may affect spinal alignment in all three dimensions Fig. 10

Fig. 10: Scoliosis. Alteration of spinal curves in 3D: coronal (A, C,D), sagittal (B) and axial planes(E).
References: Hospital of Galdácano. Radiology
Although scoliosis is usually (in 80% of cases) idiopathic,
various congenital or developmental osseous or neurologic abnormalities may lead to abnormal lateral curvatures of the spine [7].
The apex is the vertebra or disk with the greatest rotation or farthest deviation from the center of the vertebral column.
End vertebrae are those with the maximal tilt toward the apex of the curve.
Apex vertebra and end vertebra are used to measure the Cobb angle .
The Cobb angle of a scoliotic curve is the angle formed by the intersection of two lines,
one parallel to the endplate of the superior apex vertebra and the other parallel to the endplate of the inferior end vertebra.
Fig. 11
Measurement of the Cobb angle has limitations in that it is performed by using a two-dimensional radiographic image (standing AP radiograph) of a 3D deformity and does not take vertebral rotation into account
Major curve,
also called primary curve,
is the largest abnormal curve in the scoliotic spine and the first to develop.
Minor curve,
also called secondary curve,
is smaller and is considered to develop afterward,
to compensate for the perturbation of balance that accompanies the progression of major curve by repositioning the head and trunk over the pelvis to maintain balance
The terms major curve and minor curve are sometimes used as synonyms for structural curve and nonstructural curve,
respectively .
Fig. 11
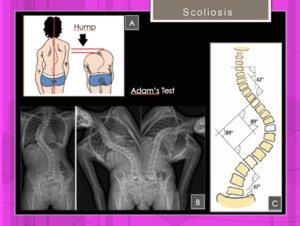
Fig. 11: Scoliosis: Structural vs non-structural spinal curves. Neutral standing AP radiograph
shows dextroscoliosis at the upper thoracic level and levoscoliosis at the thoracolumbar level (b) Rightwardbending and leftward-bending views show a correcto of the levoscoliosis, a finding indicative of a nonstructural curve. Adams test (A).
References: Hospital of Galdácano. Radiology
Nonstructural curves are corrected in Leftward-bending / Rightward-bending views. Fig. 11
Adams forward bend test: The child bends forward with the feet together and knees staright while dangling the arms.
Any imbalances in the rib cage or other deformities along the back could be a sign of scoliosis.
Fig. 11
Nash-Moe method.
Measurement of vertebral rotation.
The pedicle location on frontal radiographs is used as an indicator of the extent of vertebral rotation Fig. 12
The half vertebra on the convex side of curvature is divided into three segments,
and rotation is quantified on the basis of the pedicle location in regard to the segments

Fig. 12: Scoliosis. Rotatational assessment by the Nash-Moe method.
References: Hospital of Galdácano. Radiology
Scoliosis Classification related to characteristic clinical features:
- Infantile (age 0–3 years).
Infantile idiopathic scoliosis is a structural malformation that affects boys more commonly than girls
- Juvenile (age 4–10 years)
- Adolescent (age 11–18 years).
Adolescent idiopathic scoliosis is preponderant in girls.
The progression of idiopathic scoliosis after skeletal maturity depends on the severity of curvature.
Diagnosis:
- Radiography is the method of choice for the initial diagnostic imaging evaluation; it is sufficient to exclude most congenital and developmental osseous anomalies,
which account for most cases of scoliosis with an underlying pathologic origin.
- In cases with a complex osseous deformity, CT is mandatory,
especially when surgery is planned.
- MR imaging is used with increasing frequency to evaluate patients with an unusual curve pattern or alarming clinical manifestations
The recommended treatment:
- Adolescent idiopathic scoliosis: observation (follow-up at 4- to 12-month intervals) when the Cobb angle is less than 20°
- bracing when the Cobb angle is 20°–45° in adolescent idiopathic scoliosis
- surgery when the Cobb angle is greater than 45°
Scoliotic Attitude: In the scoliotic attitude the Cobb angle is less than 10° and lateral deviation is corrected voluntarily.
It is a condition that is due to external causes,
so that once identified and corrected this cause greatly enhances the degree of deviation.
The scoliotic attitude is classified according to the factors that cause:
- Postural
- Hysterical (have a psychological basis)
- Compensatory (Asymmetry of lower extremities and disappears in the supine decubitus position)
- Analgesic (adopt a poor posture to relieve pain)
- Inflammatory neighborhood (due to other pathologies,
for example,
appendicitis).
Adams forward bend test: Absence of a hump and vertebral rotation.
Fig. 13
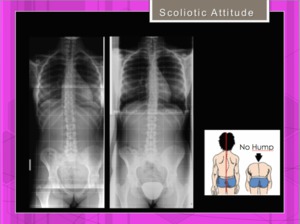
Fig. 13: Scoliotic attitude. 14y.o. girl with slight asymmetry of lower extremities. Two years later asymmetry is correcto and scoliosis is gone. Normal Adams Test.
References: Hospital of Galdácano. Radiology
SPONDYLOLISTHESIS / SPONDYLOLISIS
Spondylolisis is a condition in which there is a defect in the pars interarticularis of the vertebra.
Occurs in young athletes by repeated microtrauma,
more frequent in L5.
Fig. 14
Spondylolisis has never been seen in newborn babies: it is seen only after walking.
The initial radiograph may be normal reflecting the trend of spondylolysis to start as a phenomenon of stress and progress later to fracture. Although bone defects of typical isthmic spondylolysis run obliquely through the pars interarticularis,
and are well depicted on oblique lumbar radiography,
atypical isthmic defects have been reported
CT has higher sensitivity than X-ray in the diagnosis of the fracture.
Its high anatomic resolution enables accurate assessment of cortical margins,
but is not sensitive for detection of stress reaction due to its inability to demonstrate cortical edema.
Fig. 14

Fig. 14: Basque ball player 21y.o. Chronic back pain. Bilateral spondylolysis in L3 (X-ray and CT) and bilateral spondylolisis in L4 only seen in CT.
References: Hospital of Galdácano. Radiology
Prior to the advent of MR,
CT and SPECT imaging were considered the gold standard for diagnosis of acute injuries of the neural arch.
However,
although SPECT is highly sensitive for detection of reactive marrow changes,
it is not specific in distinguishing between acute stress reaction and complete or incomplete fracture,
and is insensitive for detection of chronic non-union.
MR has emerged as an excellent front-line test for the evaluation of back pain in adolescent athletes.
Sequences that are highly sensitive for visualization of cortical edema have enabled early detection of stress injuries or incomplete fractures of the neural arch
In the adolescent presenting for imaging evaluation of back pain,
MR sequences should be optimized for detection of marrow edema in the pars interarticularis and pedicles.
In addition to routine T1 and T2 axial and sagittal images,
sagittal short-inversion recovery time (STIR) and/or sagittal fat-saturated T2-weighted sequences should be performed .
Contiguous T2-weighted axial images should be obtained from the L4 level through the sacrum,
as well as through any other areas of interest identified on sagittal STIR or fat-saturated sequences.
A 3D gradient-echo sequence with sagittal reformatted images at the level of the facets joints is mandatory in this adolescents in order to detect bony defects (more evident in this sequence) Fig. 16
Hollenberg et al have proposed a grading system for stress injuries of the pars interarticularis based on the MR appearance [8]. Fig. 15 Fig. 16
_________________________________________________________
- Grade 0: Normal marrow signal with intact cortical margin of the isthmus
- Grade 1: Bone marrow edema with intact cortical margin of the isthmus with or without signal changes in adjacent pedicle or articular processes
- Grade 2: Incomplete fracture showing bone marrow edema and cortical breakage incompletely running though isthmus
- Grade 3:Complete fracture denoting a complete bone defect of isthmus with bone marrow edema
- Grade 4:
Fracture non-union presenting complete separation of isthmus without bone marrow edema
_________________________________________________________
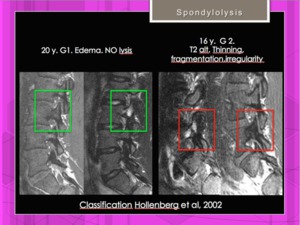
Fig. 15: MRI of spondylolysis. Hollenberg classification. Grades I and II.
References: Hospital of Galdácano. Radiology
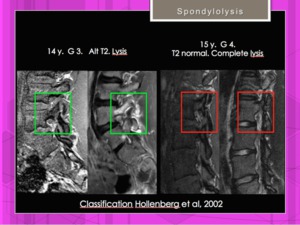
Fig. 16: MRI of spondylolysis. Hollenberg classification. Grades III and IV.
References: Hospital of Galdácano. Radiology
MRI also may be useful in prognostic decision making for these patients.
Control exams with STIR and 3D gradient-echo sequences help to evaluate the resolution ( Fig. 17 , Fig. 18 ) or the progression ( Fig. 19 ) of the spondylolisis.

Fig. 17: 15 year old soccer with constant back pain. Sagittal STIR image. High signal intensity edema withouth cortical fracture in the first MRI ( Grade 1) with resolution after a period of rest.
References: Hospital of Galdácano. Radiology
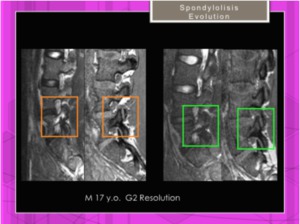
Fig. 18: Soccer. 17y.o. Sagittal STIR and 3D gradient-echo sequences. Evolution of Hollenberg Grade 2 spondylolisis with healing of the fracture and less edematous reaction.
References: Hospital of Galdácano. Radiology
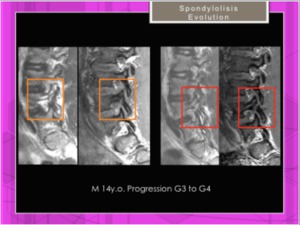
Fig. 19: Spondylolysis Grade 3 of Hollenberg in a 14 y.o. soccer player. Sagittal STIR and 3D gradient-echo sequences. Poor evolution to Grade 4 (chronic scarring without edema and more obvious fracture)
References: Hospital of Galdácano. Radiology
Spondylolisthesis is a forward slip of one vertebra relative to another.
Usually occurs in the lumbar area.
Forward slippage of an upper vertebra on a lower vertebra is referred to as anterolisthesis,
while backward slippage is referred to as retrolisthesis
Spondylolisthesis can lead to a deformity of the spine as well as a narrowing of the spinal canal (central spinal stenosis) or compression of the exiting nerve roots (foraminal stenosis).
Causes of spondylolisthesis include:
- big trauma (Traumatic Spondylolistesis)
- degenerative (Degenerative Spondylolistesis)
- tumor (Pathologic Spondylolisthesis)
- birth defect (Dysplastic Spondylolisthesis)
- repetitive sport trauma (Isthmic Spondylolisthesis)
Symptoms of spondylolisthesis include
- lower back or leg pain
- hamstring tightness,
- numbness and tingling in the legs.
The diagnosis of spondylolisthesis is based on imaging.
Usually,
it is not possible to see visible signs of spondylolisthesis by examining a patient.
Spondylolisthesis is easily identified using plain radiographs (lateral X-ray).
Meyerding grading system: Meyerding defined the slippage on plain X-ray imaging in accordance to the vertebra below[9].
The caudal vertebra is divided into four parts. Fig. 20
- Grade I is a slip of up to 25%
- Grade II is between 26%-50%.
- Grade III is between 51%-75%.
- Grade IV is between 76%-100%.
- Grade V,
or spondyloptosis,
occurs when the vertebra has completely fallen off the next vertebra.
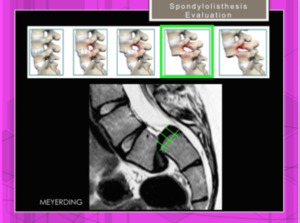
Fig. 20: Spondylolisthesis. Meyerding grading system. Example of Grade III.
References: Hospital of Galdácano. Radiology
Slip Angle: Measure angle between superior endplate of L5 and a line perpendicular to the posterior border of the sacrum Fig.
21
- normal slip angle: -10º to 0º
- Dysplasic : slip angle > 10º
- slip angle > 50º is associated with greater risk of progression
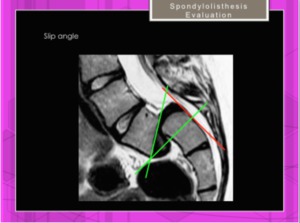
Fig. 21: Spondylolisthesis. Slip angle.Angle between superior endplate of L5 and a line perpendicular to the posterior border of the sacrum.(</= 50º)
References: Hospital of Galdácano. Radiology
Lumbar index.
This index quantifies the trapezoidal shape that L5 often assumes as the result of a high-grade slip,
the anterior vertebral body being larger than the posterior body.
The lumbar index is just the calculation of the posterior vertebral height,
divided by the anterior vertebral height,
expressed as a percentage (normal >/= 80%). However,
these values are mostly used to assess progression risk in the pediatric population.
Fig. 22
Dome-shaped sacral endplate: Dome-shaped sacral endplate is considered when the index between stright line of the sacral endplate and dome height is > 10%.
Fig. 22
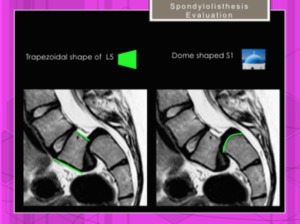
Fig. 22: Spondylolisthesis. Lumbar Index: Posterior vertebral height of L5 divided by the anterior vertebral height, expresed as a percentage. Dome-shaped sacral endplate.
References: Hospital of Galdácano. Radiology
The sacral slope is value of the angle between the superior plate of S1 and a horizontal line .
Thus a vertical sacrum is described by a low value,
a horizontal sacrum measures a high value
The pelvic incidence (PI) is a specific and constant parameter for each individual,
measured in the lumbosacral radiograph on the profile incidence,
and defined as the angle between the line connecting the midpoint of upper plateau of S1 and the centre of femoral rotation and the line perpendicular to the upper plateau of S1.
The value of PI is higher in spondylolisthesis,
increasing linearly,
according to the severity of slippage.
Fig. 23
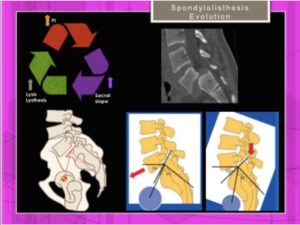
Fig. 23: Spondylolisthesis. Relationship between Pelvic Incidence, Sacral Slope and progress in spondylolisthesis and spondylolysis.
References: Hospital of Galdácano. Radiology
Predictors of slip progression have been considered:
- Female gender
- Prepubescence
- Trapezoidal L5
- Domed and vertical sacrum
- Slip angle >10º
- High grade slip (>50%)
- Inclined sacrum (>30% beyond vertical)
Other studies about the progression of the lumbosacral kyphosis and sinking of the vertebral body correlate it with cases of severe slips.
Although female gender and dysplasia (spina bifida) at the lumbosacral junction were more frequent in severe slips,
they statistically had no value in predicting progression.
A wedge form of L5 or sacral rounding also had no prognostic value.
These were secondary to the slip and expressed it but did not predict it.
The only radiologic variable with predictive value of progression was the percentage amount of the primary slip.
In age groups corresponding to the growth spurt in early puberty (girls,
9-12 years; boys,
11-14 years),
there was a tendency to progress [10]. Fig. 24
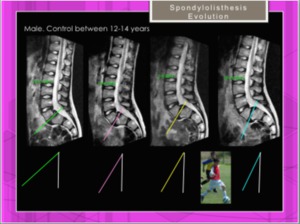
Fig. 24: Spondylolisthesis. Progression during 2 years (male, 12-14 y.o)
References: Hospital of Galdácano. Radiology
Treatment of Spondylolisthesis:
Most people with spondylolisthesis can be treated conservatively,
without the need for surgery.
Patients who fail to improve with conservative treatment may be a candidate for surgery.
Fig. 25
Management of spondylolisthesis in young people: General Rules
Fig. 25
- Asymptomatic and less than 25% slip: normal life and periodic radiographs every 6 to 8 months
- Symptomatic and less than 25% slip: physiotherapy,
avoid contact sports (rugby,
football,
karate,
etc.) and X-rays every 6 to 8 months.
- Asymptomatic and 25% to 50% slip: avoid violent exercise and gymnastics.
Radiographic control every 6 to 8 months.
- Symptomatic and 25% to 50% slip: physiotherapy,
suspend physical education for long periods of 6-12 months.
X-rays every 6 to 8 months
- About 50% slip: surgical treatment is indicated.
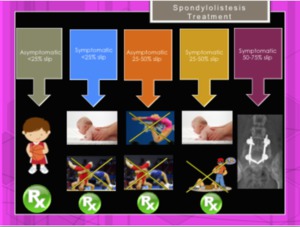
Fig. 25: Management of spondylolisthesis based on its degree of involvement: chiropractic manipulation, avoid extreme sports, and control by X-ray. Surgery is reserved to high grade lesions.
References: Hospital of Galdácano. Radiology
OTHER PATHOLOGIES
- TRAUMATIC injuries in children ( Fig. 26 )
- Strains can be caused by any low grade injury to the spine.
The most common of these is the Whiplash injury – caused by a sudden extension–flexion mechanism.
This is caused typically when a stationary person is shunted from the rear.
These athletes present with paravertebral muscle spasm,
limited range of motion and a normal neurological examination.
Radiographs demonstrate a loss in the normal cervical curvature.
There is however no evidence of injury to the spinal column and the alignment is normal.
Treatment is conservative with muscle relaxants,
physiotherapy and anti-inflammatories
- Avulsion fractures of the spinous process in the cervical spine,
also known as Clay shoveler’s fractures could be present.
- Compression fractures can occur anywhere in the vertebral column but are most common in the cervical spine from the C4 to the C7 levels and in the thoracolumbar spine from the T10 to the L2 level
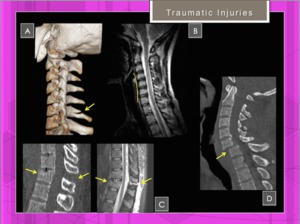
Fig. 26: Traumatic spinal injuries in young patient
References: Hospital of Galdácano. Radiology
- TUMORAL lesions in children
- EOSINOPHILIC GRANULOMA (EOG)
Includes a group of disorders characterized by a variety of tumor like lesions,
which arise from from clonal proliferation of Langerhans-
type histiocytes
Main issues:
- most common in children less than 12 years of age
- most common in the thoracic spine
- may present with progressive back pain
- vertebra plana (in 2-6 yrs old child,
EOG may present w/ collapse of single vertebra)
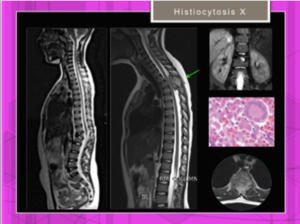
Fig. 27: Two different young patients with histiocytosis X affecting thoracic and lumbar spine.
References: Hospital of Galdácano. Radiology
lesion is usually self-limiting;Fig. 28
- at least 50% reconstitution of vertebral height may be expected;
- if there is no neurological deficit,
lesion may be followed non operatively
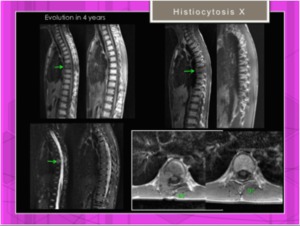
Fig. 28: Evolution of histiocytosis X: remission of the involvement of the thoracic spine.
References: Hospital of Galdácano. Radiology
The osteoid osteoma is a benign osteoblastic tumor more often in men between 7 and 25 years old.
Fig. 29
The most common clinic is predominantly nocturnal pain that improves with nonsteroidal antiinflammatory drugs (NSAIDs).
Fig. 30
Its appearance is more frequent in long bones,
but can also affect the spine,
especially the lumbar area.
The region most commonly affected is the posterior vertebral arch.
Fig. 31
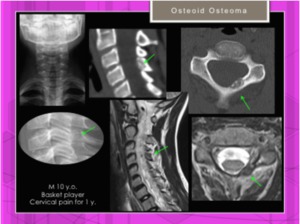
Fig. 29: Osteoid osteoma / Osteoblastoma: Bone lesion, slightly expansive in left vertebral lamina of C4 without soft tissue component.
References: Hospital of Galdácano. Radiology

Fig. 30: Periosteal osteoid osteoma in thoracic spine without periosteal reaction.
References: Hospital of Galdácano. Radiology

Fig. 31: Female. 23 yrs. Osteoid osteoma in posterior elements of L3.
References: Hospital of Galdácano. Radiology

(A) and lumbar lordosis (B)(more frequent in female References: Hospital of Galdácano. Radiology")



, sagittal (B) and axial planes(E). References: Hospital of Galdácano. Radiology")
 Rightwardbending and leftward-bending views show a correcto of the levoscoliosis, a finding indicative of a nonstructural curve. Adams test (A). References: Hospital of Galdácano. Radiology")


 and bilateral spondylolisis in L4 only seen in CT. References: Hospital of Galdácano. Radiology")


 with resolution after a period of rest. References: Hospital of Galdácano. Radiology")

 References: Hospital of Galdácano. Radiology")

 References: Hospital of Galdácano. Radiology")


 References: Hospital of Galdácano. Radiology")






