ESSR 2016 / P-0058
Hand and wrist ultrasonography: anatomy and common pathology
Congress:
ESSR 2016
Poster Number:
P-0058
Type:
Educational Poster
Keywords:
Neoplasia, Trauma, Inflammation, Education, Diagnostic procedure, Ultrasound, Neuroradiology peripheral nerve, Musculoskeletal joint, Musculoskeletal soft tissue
Authors:
S. P. Ivanoski1, B. Tolovski2, V. Vasilevska Nikodinovska2; 1Ohrid/MK, 2Skopje/MK
DOI:
10.1594/essr2016/P-0058

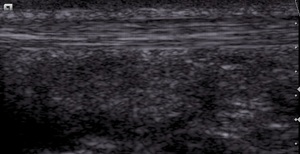
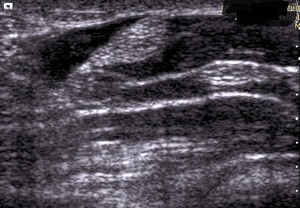
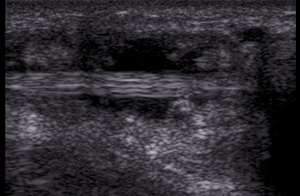
Fig. 1:
Normal flexor tendon

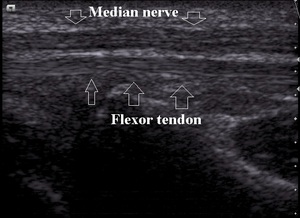
Fig. 2:
Normal flexor tendon and nerve, longitudinal view

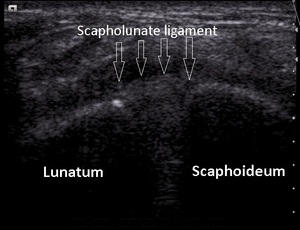
Fig. 3:
Normal scapholunate ligament

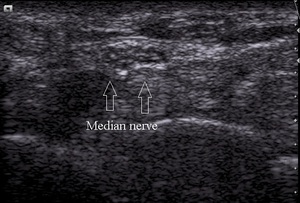
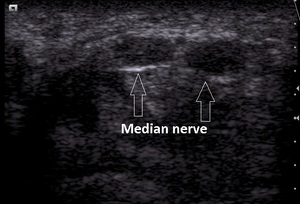
Fig. 4:
Normal median nerve-transverse view at proximal carpal tunnel level
 and longitudinal (deep part) view of normal muscles on ultrasound")
Fig. 5:
Transverse (superficial part) and longitudinal (deep part) view of normal...

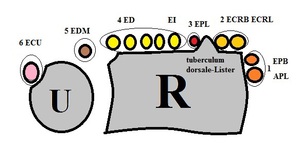
Fig. 6:
Dorsal wrist, compartments: 1 Abductor policis longus, extensor policis...

Fig. 7:
Normal dorsal wrist-transverse view
2 Extensor carpi radialis longus et...

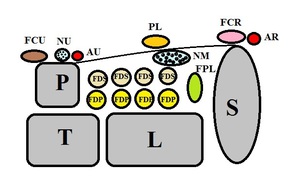
Fig. 8:
Palmar wrist: FCR- Flexor carpi radialis
FPL-Flexor policis longus
PL-...

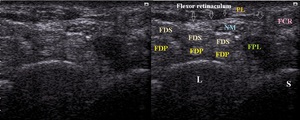
Fig. 9:
Normal palmar wrist-transverse view: FCR- Flexor carpi radialis
FPL-Flexor...

Fig. 10:
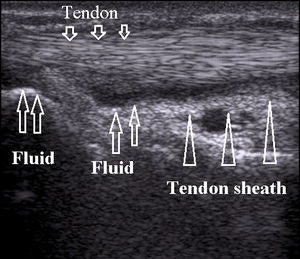
Severe tenosynovitis of flexor tendon

Fig. 11:
Tenosynovitis
")
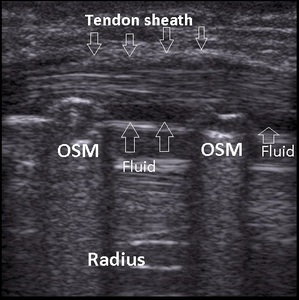
Fig. 12:
Overuse tenosynovitis due to friction with osteosynthetic material (OSM)

Fig. 13:
Extensor carpi ulnaris tendinitis

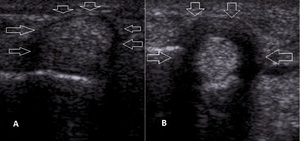
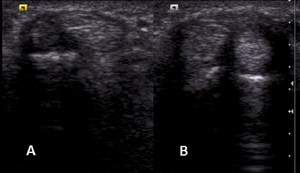
Fig. 14:
A. Normal annular ligament-A1 pulley
B. Ligament hypertrophy in trigger finger

Fig. 15:
A. Normal tendons in first extensor compartment
B. de Quervain tenosynovitis

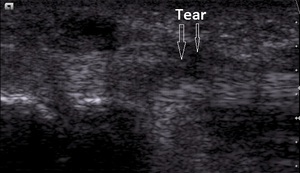
Fig. 16:
Partial thickness tear in chronic tenosynovitis

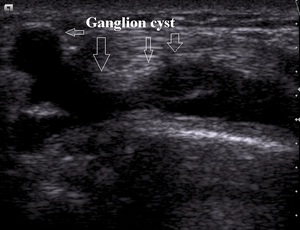
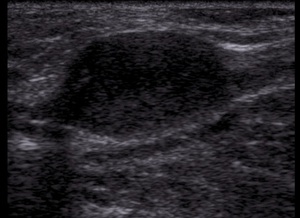
Fig. 17:
Dorsal wrist ganglion cyst

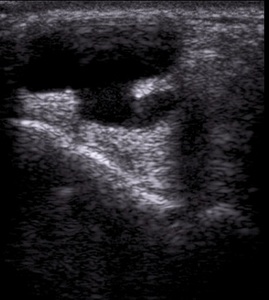
Fig. 18:
Multiseptated dorsal ganglion cyst

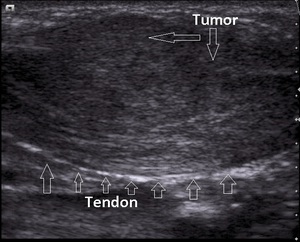
Fig. 19:
Giant cell tumor of flexor tendon sheath

Fig. 20:
Schwanomma

Fig. 21:
Carpal tunnel syndrome, axial view

Fig. 22:
Severe carpal tunnel syndrome. Cross-section area of median nerve of 24 mm2

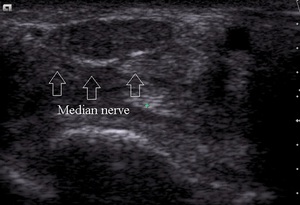
Fig. 23:
Carpal tunnel syndrome in bifid median nerve

Fig. 24:
Carpal tunnel syndrome

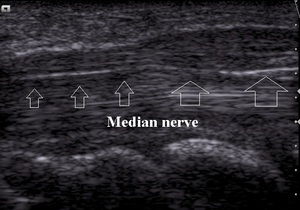
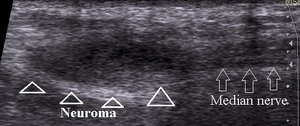
Fig. 25:
Neuroma of median nerve