Young and Burgess Classification
The Young and Burgess classification of pelvic fractures is divided into 3 distinct mechanisms of injury: anteroposterior compression,
lateral compression and vertical shear,
with a further 4th classification of combined mechanism.
Anteroposterior and lateral compression injuries are divided into 3 grades of severity.
The lower grades reflect injury to only the anterior pelvic ring with the higher grades reflecting injury to the posterior pelvis with consequent loss of stability [Burgess et al,
1990].
Injuries to the anterior part of the pelvic ring can be indicated by symphysis pubis disruption or diastasis,
or pubic rami fractures.
The posterior pelvic fractures can be fractures of the iliac bone,
the sacrum or a fracture dislocation of the sacroililiac joint,
which is the most common posterior pelvic injury [Tile and Schatzker,
2005].
Anteroposterior compression (APC)
Anteroposterior compression grade 1
This classically refers to diastasis of the pubic symphysis caused by an anteroposterior compressive force.
A study of pelvic binders has shown that their use in pelvic trauma can reduce pubic symphysis diastasis and open book fractures completely [Simpson et al,
2002].
These images demonstrate the appearances of an anteroposterior compression grade 1 injury with a pelvic binder,
when the injury to the pubic symphysis cannot be appreciated,
and without a binder in the same patient,
where there is clear diastasis.

Fig. 1: Axial Trauma protocol CT of pelvis, level of pubic symphysis. Anteroposterior compression grade 1 with pelvic binder in situ.

Fig. 2: Axial Trauma protocol CT of pelvis, level of pubic symphysis. Anteroposterior compression grade 1, without pelvic binder (same patient as in Figure 1).
There is no disruption of the sacroiliac complex,
therefore this is a stable fracture,
although the patient may go on to have operative fixation of the diastasis [Guthrie et al,
2010].
Anteroposterior compression grade 2
Grade 2 anteroposterior compression injury includes widening of the symphysis pubis with additional widening of the anterior part of the sacroiliac joint.
Injury to the ipsilateral anterior sacroiliac ligaments,
sacrotuberous and sacrospinous ligaments occurs with widening of the sacroiliac joint anteriorly.
The stronger posterior sacroiliac ligaments will remain intact [Tile and Schatzker,
2005]. This fracture pattern is commonly described as 'open book'.
As noted for Anteroposterior compression grade 1 injuries the use of pelvic binders can reduce these fractures and make them more difficult to identify.
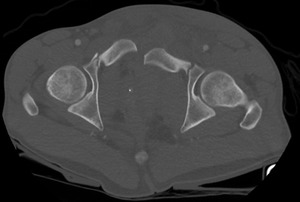
Fig. 3: Axial Trauma protocol CT of pelvis, level of pubic symphysis. Anteroposterior compression grade 2.

Fig. 4: Axial Trauma protocol CT of pelvis, level of sacroiliac joints. Anteroposterior compression grade 2.
These axial CT images show widening and disruption of the pubic symphysis,
with posterior displacement of associated fractures of the pubic rami bilaterally.
Comparing the left sacroiliac joint (arrow) with the right we can see anterior widening of the sacroiliac joint.
These appearances indicate a potentially unstable pelvis.
Knowledge of the expected fracture pattern will allow you to identify this injury,
which can be subtle.
Note that the posterior joint margin remains symmetrical with the right,
indicating that the posterior sacroiliac ligaments are intact.
Anteroposterior compression grade 3
Grade 3 anteroposterior compression fractures of the pelvis will incorporate pubic symphysis disruption but unlike the grade 2 injury there will be disruption of the entire left sacroiliac joint.
This will mean that there is a 'floating' hemipelvis on the side of injury,
completely separated from the sacrum with complete disruption of the posterior sacroiliac ligaments.
These injuries are often associated with significant vascular injury [Burgess et al,
1990].
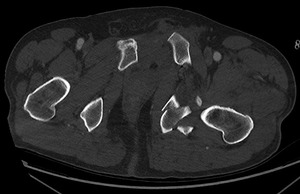
Fig. 5: Axial Trauma protocol CT of pelvis, level of pubic symphysis. Anteroposterior compression grade 3.

Fig. 6: Axial Trauma protocol CT of pelvis, level of inferior sacroiliac joints. Anteroposterior compression grade 3.

Fig. 7: Axial Trauma protocol CT of pelvis, level of superior sacroiliac joints. Anteroposterior compression grade 3
As in grade 2 injury there is diastasis of the pubic symphysis with obvious widening of the sacroiliac joints anteriorly.
However,
at the caudal margin of the sacroiliac joints there is a more subtle area of sacroiliac joint disruption (arrow) at the posterior sacroiliac joint.
Although a subtle injury (with the pelvic binder in situ) the posterior sacroiliac joint cannot be disrupted without significant injury to the posterior sacroiliac ligaments,
therefore this indicates an unstable grade 3 Anteroposterior compression injury.
Vertical shear (VS)
Vertical shear fractures are not graded,
however a vertical shear conforming to the classic description indicates an unstable fracture in itself as there will be vertical displacement of the ipsilateral hemipelvis relative to the sacrum and contralateral hemipelvis, with both anterior and posterior diastasis.
The anterior injury can be at the pubic symphysis or pubic rami but vertical displacement will help separate from APC or LC type injury.
This is often more easily appreciated on coronal or 3D reconstruction.
The posterior injury will often be though the sacroiliac joint but can also be through the sacrum or iliac.

Fig. 8: Axial Trauma protocol CT of pelvis, level of sacroiliac joints. Vertical shear.

Fig. 9: Coronal reconstruction of trauma CT in patient with Vertical shear injury.
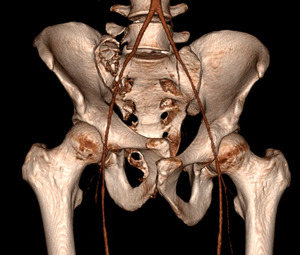
Fig. 10: 3D reconstruction of trauma CT in patient with Vertical shear injury.
This case demonstrates fractures passing through the right sacral ala,
with vertical displacement of the fracture on coronal reconstruction.
Note also the fracture of the right L5 transverse process,
onto which the iliolumbar ligament attaches,
another key stabiliser of the pelvis [Guthrie et al,
2010].
The 3D reconstruction also demonstrates clearly the vertical disruption of the pubic symphysis.
Although the right sacroiliac joint is intact the vertical disruption of the sacral fracture indicates complete disruption of the posterior part of the pelvic ring.

Fig. 11: AP plain radiograph of Vertical shear injury after fixation.
Post operative plain radiograph demonstrates cannulated screw fixation across the righ sacral alar fracture.
There is also anterior fixation of the pubic symphysis.
Lateral compression (LC)
Lateral compression grade 1
In fractures due to lateral compression the impacted hemipelvis will rotate medially.
In a grade 1 injury this will cause transverse fractures of the pubic rami,
with a lateral compression fracture of the sacrum.
There is no posterior ligamentous injury or inherent instability to this fracture pattern.

Fig. 12: Axial Trauma protocol CT of pelvis, level of inferior pubic rami. Lateral compression grade 1.

Fig. 13: Axial Trauma protocol CT of pelvis, level of sacroiliac joints. Lateral compression grade 1.
These images show the transverse fracture of the right inferior pubic ramus,
with consequent minor medial displacment of the medial fracture fragment.
Fracture of the right superior pubic ramus was visible on other slices of the trauma scan.
The 2nd image is from a different patient and demonstrates the classic sacral compression fracture,
indicating a lateral compression injury.
This plain radiograph demonstrates the appearances of a lateral compression grade 1 injury.
The right-sided pubic rami fractures are visible on the plain pelvic radiograph.
The associated sacral injury cannot be definitively identified on radiograph.

Fig. 14: AP Plain radiograph of pelvis in patient with Lateral Compression grade 1 injury.
On axial STIR (Short Tau Inversion Recovery) MRI we can see that there is also a fracture of the right sacral alar consistent with a grade 1 lateral compression injury.
In addition there is bone marrow oedema in the posterior iliac bone,
consistent with bone contusion,
although no displaced fracture to indicate a higher grade lateral compression injury.
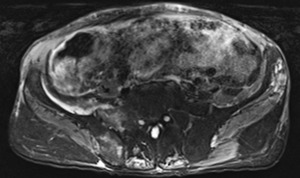
Fig. 15: Axial STIR sequence MRI of pelvis at level of sacroiliac joint in patient with Lateral Compression grade 1 injury.
Lateral compression grade 2 injury
In a grade 2 injury there will be the same fractures seen in a grade 1 lateral compression injury,
with the addition of a fracture of the ipsilateral iliac wing.
The fracture of the iliac wing tends to occur just anterior to the sacroiliac joint,
as the strong posterior sacroiliac joints will usually keep the iliac in situ at the sacroiliac joint,
forming a crescent fracture [Burgess et al,
1990].
As these fractures involve an iliac wing fracture through the posterior ring they will usually be fixed in order to stabilise the pelvis.
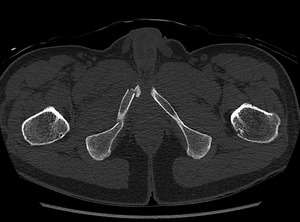
Fig. 16: Axial Trauma protocol CT of pelvis, level of inferior pubic rami. Lateral compression grade 2.
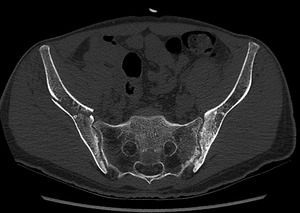
Fig. 17: Axial Trauma protocol CT of pelvis, level of sacroiliac joints. Lateral compression grade 2.

Fig. 18: AP Plain radiograph of Lateral compression grade 2 injury.
This case demonstrates the right sided pubic rami fractures and characteristic right iliac crescent fracture.
Note that on the plain radiograph of the same patient the pubic rami fractures are obvious,
but the iliac fracture is much more difficult to define.
Lateral compression grade 3
In high impact injury the internal rotation of the ipsilateral hemipelvis will continue,
causing forced external rotation of the contralateral pelvis.
This is known as a 'windswept pelvis'.
There will be disruption to the pelvic ring in both hemipelvises,
causing bilateral instability.
The LC grade 3 description does not necessarily indicate disruption and displacement of the posterior ring and therefore these injuries may be desribed as 'partially stable' rather than 'completely unstable' if the posterior sacroiliac ligaments are still intact [Tile and Schatzker,
2005].

Fig. 19: Axial Trauma protocol CT of pelvis, level of sacroiliac joints.Lateral compression grade 3.

Fig. 20: Coronal reconstruction of Trauma protocol CT of pelvis, level of superior pubic rami. Lateral compression grade 3.
In this severe grade 3 LC injury we can see that there is internal rotation of the left hemipelvis with external rotation of the right hemipelvis and widening of the right anterior sacroiliac joint.
The sagittal reconstruction demonstrates associated overriding of the pubic rami at the pubic symphysis.
However,
there is also a comminuted fracture-dislocation at the left sacroiliac joint indicating complete instability of the left sacroiliac joint and a floating hemiplevis on the left.

Fig. 21: AP plain radiograph of Lateral compression grade 3 injury after operative fixation.
On the post operative radiograph we can see there has been fixation of both sacroiliac joints,
with a cannulated screw spanning both joints.
In addition there has been fixation of the left iliac fracture and across the pubic symphysis.
Combined mechanism (CM)
In combined mechanism there will be a combination of at least 2 of the other injury patterns.
The combined mechanism classification by itself iwll not imply instability.
Therefore it is important to study which injury patterns are present and then determine where related fractures or displacement will cause instability.
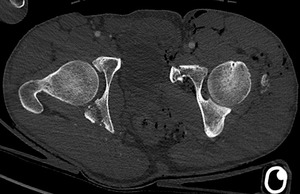
Fig. 22: Axial Trauma protocol CT of pelvis, level of acetabula. Combined mechanism.

Fig. 23: Axial Trauma protocol CT of pelvis, level of sacroiliac joints. Combined mechanism.

Fig. 24: Coronal reconstruction of Trauma protocol CT of pelvis, level of superior pubic rami. Combined mechanism.
The axial images shows comminuted fractures of the left pubic ramus and left iliac bone,
with internal rotation of the left hemipelvis,
consistent with a grade 2 lateral compression injury.
On coronal reconstruction however there is also vertical displacement of the superior pubic rami at the pubic symphsis.
In addition there are superiorly avulsed fragments of bone visible on the left with considerable soft tissue disruption and subcutaneous air.
The appearances are consistent with an open fracture due to combined mechanism of lateral compression and vertical shear.
This MRI demonstrates a further case of combined mechanism injury.
On the axial STIR sequence there can be seen bilateral superior pubic rami fractures,
which would be consistent with an AP compression injury.
On the coronal STIR sequence we can see a vertical fracture through the sacrum.
This is not vertically displaced and is consistent with a lateral compression injury.
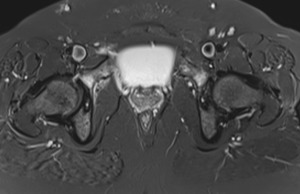
Fig. 25: Axial STIR sequence MRI of Combined Mechanism injury at level of superior pubic rami.
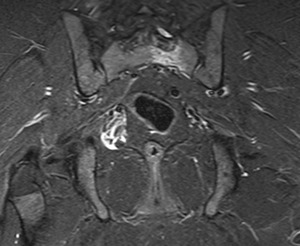
Fig. 26: Coronal STIR sequence MRI of Combined Mechanism injury at level of superior sacroiliac joints.
Associated injuries with pelvic fractures
In this combined mechanism injury the coronal CT reconstruction of the pubic symphysis indicates vertical displacement through the symphysis consistent with vertical shear mechanism.
The axial images of the sacroiliac joint demonstrate a comminuted,
posteriorly displaced fracture of the left iliac wing extending into the sacroiliac joint.
This is consistent with anteroposterior compression mechanism.
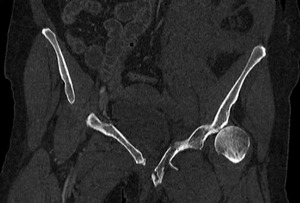
Fig. 27: Coronal reconstruction of Trauma protocol CT of pelvis, level of pubic symphysis. Combined Mechanism.

Fig. 28: Axial Trauma protocol CT of pelvis, level of sacroiliac joints. Combined mechanism.
Axial CT on soft tissue windows clearly delineates gross soft tissue swelling and haematoma anteriorly to the left sacroiliac joint.
Internally there are several blushes of contrast indicating active extravasation.
While contrast can be seen in the right internal and external iliac vessels these structures cannot be defined on the left and this patient had significant vascular injury at surgery.
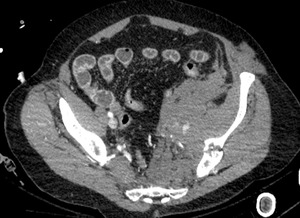
Fig. 29: Axial Trauma protocol CT of pelvis, soft tissue reconstruction, level of iliac bones. Combined mechanism.
On this axial CT on bone reconstruction there is a lateral compression grade 3 injury of the pelvis.
Axial CT of the pubic symphysis shows overriding of the symphysis,
while there is a subtly displaced fracture traversing the body of the sacrum.

Fig. 30: Axial Trauma protocol CT of pelvis, level of pubic symphysis. Lateral compression grade 3.
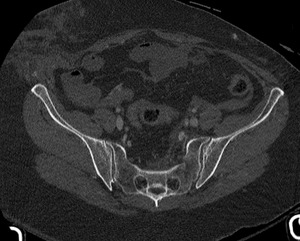
Fig. 31: Axial Trauma protocol CT of pelvis, level of sacroiliac joints. Lateral Compression grade 3.
On the soft tissue windows of the same patient,
slightly superiorly to the pelvis,
there is haematoma in the right paracolic gutter.
There are blushes of contrast within this haematoma,
as well as adjacent to the mesenteric vessels.
The right sided bowel is hypo-enhancing relative to the left sided bowel and these appearances are consistent with significant mesentery and bowel injury,
confirmed at surgery.
There is also a traumatic tear of the right sided abdominal muscles with herniation of intra-abodminal fat.
The pattern of these right sided abdominal injuries is consistent with the lateral compression injury indicated by the pattern of bone injury.

Fig. 32: Axial Trauma protocol CT of pelvis, soft tissue reconstruction, level of L5. Lateral compression grade 3.
