Until recently,
the definitive diagnosis of spondyloarthritis (SpA) relied on conventional radiography.
Studies have compared MR imaging and conventional radiography revealing strengths and weaknesses of both modalities.
Results suggested that syndesmophytes are better depicted with conventional radiography; ankylosis,
equally well with both imaging techniques; and all other lesions,
better with MR imaging.
Thus,
MRI is a more sensitive method to depict the characteristic findings of spondylarthropathies.
Furthermore,
radiographic changes usually develop at least 5 years after symptom onset.
In fact,
for many years,
the diagnose of axial spondylarthritis after clinical and biochemical evaluation was delayed as it was determined by the presence of sacroiliitis on radiography.
Conventional radiography can only capture post-inflammatory structural changes and is unable to depict early inflammatory lesions in the sacroiliac joints and thus the definitive diagnose was only possible after established disease.
Diagnostic criteria for spondyloarthritis proposed by the Assessment of Spondyloarthritis International Society (ASAS) for patients younger than 45 years with low back pain for more than 3 months are:
- MRI or conventional radiography with sacroiliitis and at least one clinical finding
- Positive HLA-B27 result and at least two clinical findings
Clinical findings:
- Inflammatory back pain
- Arthritis
- Enthesitis (Achilles)
- Uveitis
- Dactylitis
- Psoriasis
- Crohn colitis
- Family history of spondyloarthropathy
- Positive HLA-B27 result
- Good response to non-steroidal anti-inflammatory drugs
- Positive C- reactive protein result.
According to the classification criteria,
MRI of sacroiliitis combined with at least one specific clinical feature in a young adult with chronic back pain has 97.2% sensitivity and 94.2% specificity for the diagnosis of axial spondyloarthritis.
The MORPHO definition of a ‘positive’ sacroiliac joint on MRI:
- Bone marrow edema (BME) according to the ASAS definition
- Erosions in at least two SIJ quadrants on the same MRI slice or in a single SIJ quadrant on at least two consecutive MRI slices
- BME and erosions in at least one quadrant each (not necessarily on the same MRI slice)
A “positive” spinal MRI for axial spondylarthropathies:
- Anterior/posterior spondylitis (vertebral corner inflammatory lesions) at 3 sites -highly suggestive
- Vertebral corner fat infiltration (if a great number of lesions are present) - highly specific.
MRI in Spondylarthropathies
MRI is the most sensitive method to detect active sacroiliitis,
in fact,
it is superior to scintigraphy,
computed tomography (CT) and radiography in patients suggestive to have spondylarthritis who show normal or equivocal SIJ changes.
Changes in spondyloarthritis may be very subtle and a good protocol should be used.
Structural damage and chronic lesions,
such as fatty degeneration and erosions,
are best visualized on T1-weighted images.
For assessment of the sacroiliac joints,
coronal and axial oblique images in the plane of the sacroiliac joints should be used.
T1- and T2-weighted sequences with fat suppression or STIR sequences are recommended.
If gadolinium administration is performed,
T1-weighted sequences with fat suppression can be performed in the coronal or axial oblique planes.
The major advantage of MRI is its ability for detailed assessment of all structures such as synovial membrane,
cartilage,
joint capsule,
entheses,
ligaments,
tendons and bone,
with high spatial resolution and good contrast.
In fact,
MRI can provide not only detailed structure visualization but also the information on both disease activity and structural damage in the same examination.
It may also allow a quantification of inflammation and structural damage of the SIJ,
which provide a more detailed assessment of MRI abnormalities and their changes over time.
Although it is now considered the most sensitive method to evaluate SIJ,
MRI is not specific for SpA and BME on SIJ can be present in healthy subjects.
Spine alterations are also not specific to SpA,
with inflammation and fat infiltration being also present in patients with degenerative spinal disease (a very common etiology among subjects with chronic back pain).
Imaging Features
- Spinal changes associated with spondyloarthritis are:
- Romanus lesion - anterior spondylitis
- Andersson lesion – diskitis
- Ankylosis
- Syndesmophytes
- Insufficiency fractures
- Enthesitis of the interspinal ligaments
- Arthritis of the apophyseal and costovertebral joints.
Romanus lesions are the earliest changes of spondylitis that can be depicted on conventional radiographs and consist in erosions or radiolucent lesions involving the anterior and posterior edges of the vertebral endplates and evolve to the so called “shinny corners” on x-ray due to,
sclerotic lesions of the edges of the vertebral endplates.
At MRI they are characterized by low signal intensity of the rim of the endplate on T1-weighted images and as high signal intensity on STIR images that represent BME or osteitis (stage not seen on conventional radiographs).
Later,
the epiphyseal ring become hyperintense on T1-weighted images,
representing areas of postinflammatory fatty bone marrow degeneration.
(stage corresponding to the “shiny corners” described on conventional radiographies).
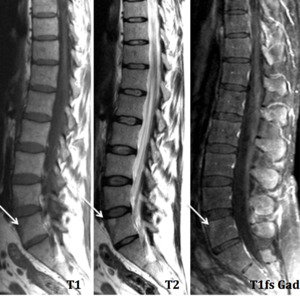
Fig. 1: Lumbar Spine –Sagital – Romanus lesion (L5) – “shining corner” in water sensitive sequence (T2) in a patient HLA B27+ with family history of ankylosing spondylitis
References: Hospital de São João, Porto
Andersson lesion corresponds to the inflammatory,
non-infectious,
involvement of the intervertebral disks (spondylodiskitis).
At conventional radiography they are only recognized as irregularities of the vertebral endplates that spare the anterior and posterior edges and evolve mainly the central part.
These alterations correspond to later findings in the course of the disease.
On the other hand,
with MRI examination early findings can be seen.
Disk-related signal-intensity abnormalities of one or both vertebral halves that can appear hyperintense on STIR images and hypointense on T1-weighted images.
Lines of increased signal intensity may be seen at the interface between the anulus fibrosus and nucleus pulposus.

Fig. 2: T1-weighted image + gad – Vertebral epiphysitis and diskitis – contrast uptake (arrow)
References: Hospital de São João, Porto
Ankylosis can involve either the center or the edges of the vertebral body and correspond to bony extensions through the disk.
It is thought that the bony extensions localized at the anterior and posterior edges results from the volution of Romanus lesions and that the central bony extension results form Andersson lesions.
The newly formed bone has the same signal intensity as normal bone on MR images.
Syndesmophytes are bony outgrowths of the anterior vertebral edges that are typically associated with ankylosing spondylitis.
As they are bony structures,
conventional radiographs and CT appear to be superior to MRI in their depiction and can be hyper or hypo intense on STIR images depending of the phase of the disease.

Fig. 3: Lumbar x-ray (AP view) and T2-w fat sat, coronal MRI – paravertebral ligament ossification of the anterior vertebral edges
References: Hospital de São João, Porto

Fig. 4: Lumbar x-ray (lateral view) and T1-w sagittal MRI – paravertebral ligament ossification of the anterior vertebral edges
References: Hospital de São João, Porto
Insufficiency fractures correspond to the non-inflamatory type of Andersson lesion.
They can occur either spontaneously or after minimal trauma,
often on the basis of prior osteoporotic spine,
usually associated with ankylosing spondylitis.
Insufficiency fractures occur as fatigue fractures at the level of the disk (transdiskal) or at the level of the vertebral body (transvertebral).
Conventional radiograph often suffice to make a correct diagnosis.
At MRI,
they are typically hypointense on T1-weighted images and as they become older they become hyperintense on T1-weighted images.
Enthesitis corresponds to the inflammatory alterations of the stabilizing ligaments of the spine.
The interspinal ligaments and the supraspinal ligaments are those that are more frequently involved and appear hyperintense on either STIR images or contrast-enhanced T1-weighted fat-saturated images.
At T1-weighted images the ligaments involved appear thickening.
These inflammatory changes can be associated with osteitis of the spinous processes (also characterized by high signal intensity on STIR images).
Conventional radiographs can demonstrate only indirect signs of this type of lesion being usually missed with this type of examination.
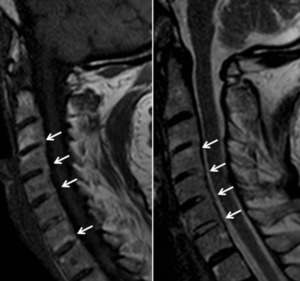
Fig. 5: MRI T1 and T2-w sagittal images – Posterior longitudinal ligament inflammation (enthesitis)
References: Hospital de São João, Porto
Arthritis of the apophyseal and costovertebral joints are comparable to arthritis of peripheral joints in terms of imaging features.
They are characterized by joint effusion,
synovitis,
erosions,
and bone marrow edema.
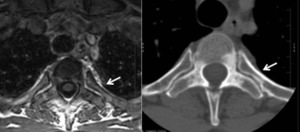
Fig. 6: MRI axial T1-w and CT axial costovertebral junction – Bone marrow (MRI) and mineral changes (CT) due to arthritis
References: Hospital de São João, Porto
Sacroiliac joint changes are usually associated with:
- Bone marrow edema
- Synovitis and capsulitis
- Enthesitis
- Subchondral sclerosis
- Erosions
- Fat deposition
- Ankylosis
The correct assessment of the sacroiliac joints should comprise coronal and axial oblique images in the plane of the sacroiliac joints - T1- and T2-weighted sequences with fat suppression or STIR sequences.
If gadolinium administration is performed,
T1-weighted sequences with fat suppression can be performed in the coronal or axial oblique plane.
Bone marrow edema is characterized as high signal intensity on STIR images and fat-suppressed contrast- enhanced T1-weighted images.
The typical location of the edema is periarticularly or on subchondral bone surfaces of the sacroiliac joints and is usually bilateral and symmetric appearing most commonly in the lower and posterior thirds of the joints.
When the edema is unilateral,
infectious sacroiliitis must be excluded.
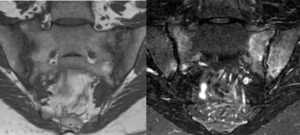
Fig. 7: MRI Coronal T1 and STIR– Sacroiliitis- Low signal in T1 and high signal in STIR in both sides of sacroiliac joints
References: Hospital de São João, Porto
Synovitis and capsulitis are exposed by high signal intensity in the synovial or anterior and posterior capsules of the sacroiliac joints,
respectively,
on fat-sat contrast-enhanced T1-weighted images.
Enthesitis is characterized by high signal intensity at the junctional area between bone and tendons,
fascia,
ligaments or capsules on STIR images and fat-suppressed contrast-enhanced T1-weighted images.
The high signal intensity may extend to adjacent bone marrow and surrounding soft tissue.
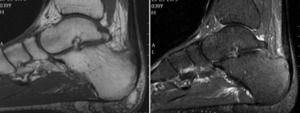
Fig. 8: Ankle- sagital T1 and T2 fat sat. Spondyloarthropathy peripheral involvement. Achilles tendinitis, paratendinitis and enthesitis – Thickening of Achilles tendon with edema at the surrounding fat, bone marrow edema and cystic changes at calcaneal tendon insertion.
References: Hospital de São João, Porto
Subchondral sclerosis corresponds to slerotic areas on both joint sides.
The iliac and sacral surfaces are depicted as areas of low signal intensity on STIR and T1-weighted images.
They typically do not enhance on fat-suppressed contrast-enhanced T1-weighted images and extends at least 5 mm from the sacroiliac joint surface.
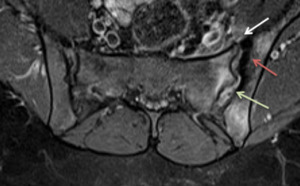
Fig. 9: Axial MRI T1-w + gad – Enthesitis (white arrow), subchondral sclerosis (red arrow) and synovitis (green arrow)
References: Hospital de São João, Porto
Erosions are bony defects at the joint surface that appear as areas of low signal intensity on T1-weighted images and may occur throughout the cartilaginous compartment of the joint.
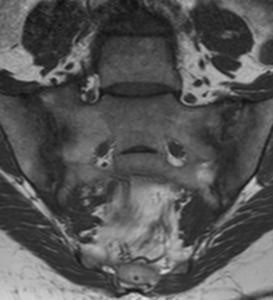
Fig. 10: MRI coronal T1 – Marginal erosions in both sides of the SIJs
References: Hospital de São João, Porto
Bone fat depositions present as increased signal intensity in periarticular bone marrow on T1-weighted images.
This finding is nonspecific and often indicates areas of previous inflammation in a patient with spondyloarthritis as described prior at Romanus lesions.
Ankylosis corresponds to bony extensions that fuse the bone surfaces to form bony bridges across the joint.
MRI reveals the same signal intensity of the adjacent bone marrow and is sometimes surrounded by areas of fatty degeneration of high signal intensity on T1-weighted images.
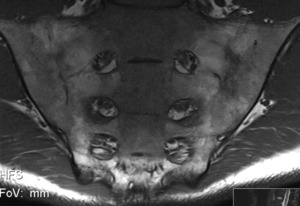
Fig. 11: MRI coronal T1-w – Effacement of the joints and fatty bone marrow transformation
References: Hospital de São João, Porto
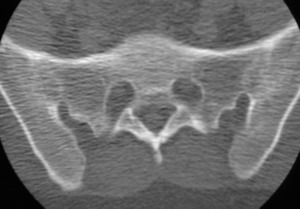
Fig. 12: CT coronal – Bony ankylosis
References: Hospital de São João, Porto
The ASAS diagnostic criteria for spondyloarthritis include MRI of only the sacroiliac joint,
but the identification of spinal inflammatory lesions supports the diagnosis.
Differential Diagnosis
Degenerative Sacroiliitis
Degenerative changes of the sacroiliac joints are characterized by anterior and middle thirds alterations with irregularity and narrowing of the articular space,
periarticular bone sclerosis,
subchondral cysts,
and the absence of inflammatory features such as erosions or BME.
Other degenerative alterations of the adjacent articular surfaces are commonly seen.
Infectious Sacroiliitis
Infectious sacroiliitis is usually characterized by unilateral involvement with high signal intensity of the subchondral bone surfaces of the SIJ on STIR images and fat- suppressed contrast-enhanced T1-weighted images accompanied of inflammation of the surrounding soft tissue.
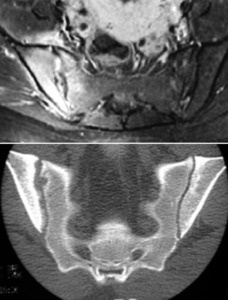
Fig. 13: MRI T1-w fat sat + gad – Periarticular enhancement with enlargement of the joint space and synovitis with periarticular inflammatory changes. CT coronal – Erosions and asymmetry of the SIJ with sclerosis of the iliac side (right).
References: Hospital de São João, Porto
Osteitis Condensans Ilii
Osteitis condensans ilii corresponds to a localized unilateral or bilateral triangular area of sclerosis on the ilium adjacent to the sacroiliac joint,
typically seen in multiparous women.
On MRI it is characterized by a triangular area of low signal intensity on T1-weighted images of the medial portion of the ilium adjacent to the anterior and middle thirds of the sacroiliac joints.
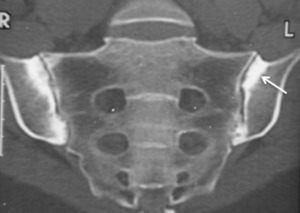
Fig. 14: CT coronal - Osteitis condensans ilii
References: Hospital de São João, Porto
Osteophytes of Lumbar Osteoarthritis
Osteophytes are usually confused with the syndesmophytes.
Osteophytes are characterized by horizontal initial bone proliferation extending the vertebral plate that is followed by the formation of bony bridges between the vertebral corners.
The presence other degenerative alterations as bone sclerosis and subchondral cysts and the absence of inflammatory alterations suggest osteoarthritis.
Modic Lesion
Modic lesions are usually associated with degenerative changes of the intervertebral disks,
although these features can also be found in Andersson lesions (however,
Andersson lesions are commonly associated with other findings suggestive of spondyloarthritis).
Incorrect differentiation between Modic and Andersson lesions is a common pitfall in the diagnosis of spondyloarthropathies.
Modic lesions corresponds to the degeneration of the vertebral endplate and can be classified as type 1 or 2.
Type 1 Modic lesion present as hypointensity on T1-weighted images and hyperintensity on T2-weighted images,
representing bone marrow edema and inflammation.
Type 2 Modic changes are associated with the conversion of normal red hematopoietic bone marrow to yellow fatty marrow and are hyperintense on T1-weighted images and isointense or slightly hyperintense on T2-weighted images.
Infectious Spondylodiskitis
Andersson lesions should also be differentiated from infectious spondylodiskitis.
The later is characterized by inflammatory changes of the vertebral plates visualized as high signal intensity on STIR images and fat-suppressed T2-weighted images,
usually in association with paravertebral and epidural soft-tissue.
The presence of a paraspinal or epidural collection should also orient the diagnosis toward an infectious process.

 – “shining corner” in water sensitive sequence (T2) in a patient HLA B27+ with family history of ankylosing spondylitis References: Hospital de São João, Porto")
 References: Hospital de São João, Porto")
 and T2-w fat sat, coronal MRI – paravertebral ligament ossification of the anterior vertebral edges References: Hospital de São João, Porto")
 and T1-w sagittal MRI – paravertebral ligament ossification of the anterior vertebral edges References: Hospital de São João, Porto")
 References: Hospital de São João, Porto")
 and mineral changes (CT) due to arthritis References: Hospital de São João, Porto")


, subchondral sclerosis (red arrow) and synovitis (green arrow) References: Hospital de São João, Porto")



. References: Hospital de São João, Porto")
