ESSR 2017 / P-0306
Traumatic overuse injuries in athletes: An observational nonrandomised prospective study with multimodality imaging and follow up
Congress:
ESSR 2017
Poster Number:
P-0306
Type:
Scientific Poster
Keywords:
Trauma, Inflammation, Athletic injuries, Imaging sequences, Diagnostic procedure, Arthrography, Ultrasound, SPECT-CT, MR, Musculoskeletal soft tissue, Musculoskeletal joint, Emergency
Authors:
D. Dalili, T. M. Bansal, N. Khandwalla, Z. Shah, M. George, M. J. Bankes, A. Isaac; London/UK
DOI:
10.1594/essr2017/P-0306

Fig. 1:
Achilles tendon rupture: lateral tibia/fibula radiograph

Fig. 2:
Achilles tendon rupture: lateral radiograph of left ankle

Fig. 3:
Achilles tendon rupture: AP radiograph of Left ankle

Fig. 8:
Lateral left ankle radiograph post operative achilles tendon repair, note the...

Fig. 12:
Anterior inferior talar fracture impaction injury: Lateral left ankle radiograph

Fig. 16:
Fifth MT base apophysitis AP radiograph of the left foot

Fig. 17:
Fifth MT base apophysitis Lateral radiograph of the left foot

Fig. 24:
Chronic adductor avulsion and myositis ossificans: AP pelvis radiograph

Fig. 25:
Chronic adductor avulsion and myositis ossificans: Oblique pelvis radiograph

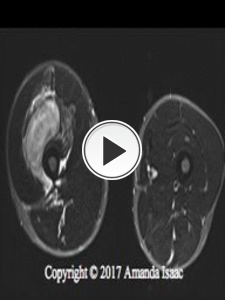
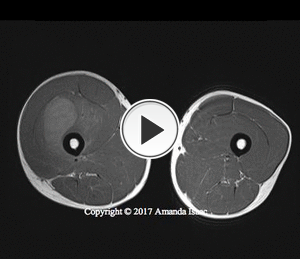
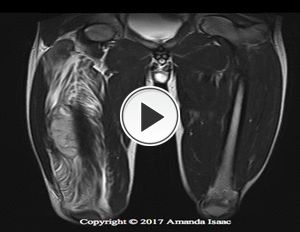
Fig. 33:
Compartment syndrome in a rugby player: AP radiograph of right femur

Fig. 34:
Compartment syndrome in a rugby player: lateral radiograph of right femur

Fig. 40:
Compartment syndrome in a rugby player: Intra-operative findings, demonstrating...

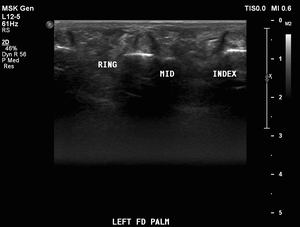
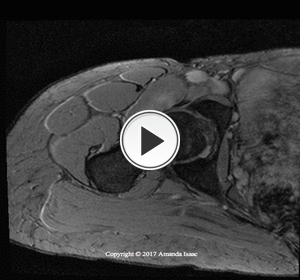
Fig. 41:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 42:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 43:
A young violinist complaining of pain in his digits and hand: Ultrasound...

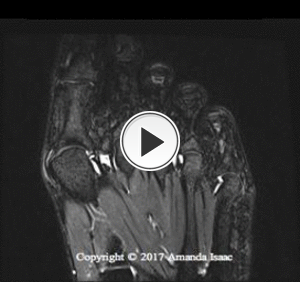
Fig. 44:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 45:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 46:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 47:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 48:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 49:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 50:
A young violinist complaining of pain in his digits and hand: Ultrasound...

Fig. 58:
Hallux valgus MCL big toe sprain and grade II injury: weight bearing AP view of...

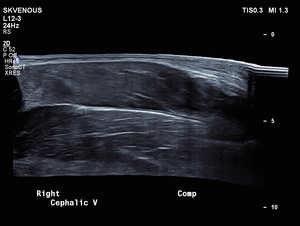
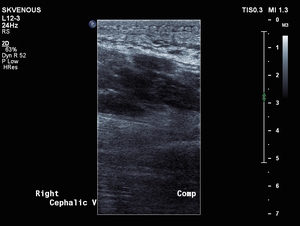
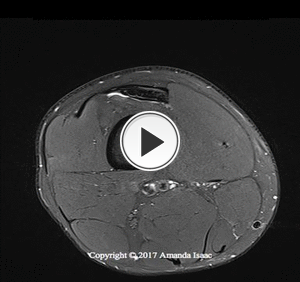
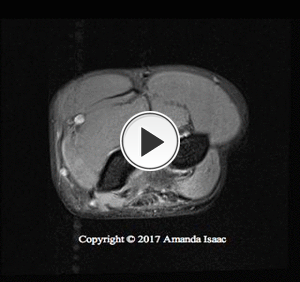
Fig. 60:
Isolated long head triceps injury US

Fig. 61:
Isolated long head triceps injury US

Fig. 62:
Isolated long head triceps injury US

Fig. 63:
Isolated long head triceps injury US

Fig. 66:
Young athletics competitor: Jumper partial avulsion of the patellar tendon: AP...

Fig. 67:
Young athletics competitor: Jumper partial avulsion of the patellar tendon:...

Fig. 71:
Syndesmotic rupture in a Rugby player: AP plain radiograph of the ankle

Fig. 72:
Syndesmotic rupture in a Rugby player: lateral plain radiograph of the ankle

Fig. 78:
Long distance marathon runner with a right femoral stress fracture: AP pelvis...

Fig. 79:
Long distance marathon runner with a right femoral stress fracture: lateral...

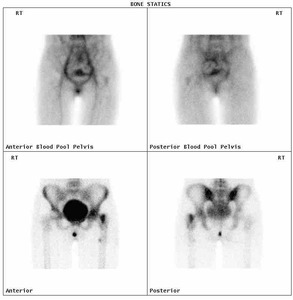
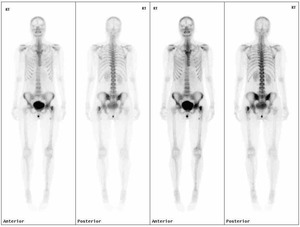
Fig. 80:
Long distance marathon runner with a right femoral stress fracture:...

Fig. 81:
Long distance marathon runner with a right femoral stress fracture:...

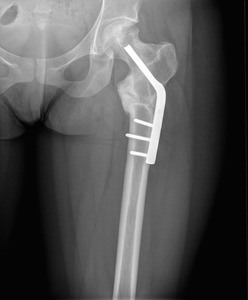
Fig. 82:
Long distance marathon runner with a right femoral stress fracture: Post...

Fig. 83:
Long distance marathon runner with a right femoral stress fracture: Post...

Fig. 93:
Stress fracture in the left femur: AP radiograph of the pelvis

Fig. 94:
Stress fracture: lateral radiograph of the left femur

Fig. 95:
stress fracture in 12 year old intraoperative imaging

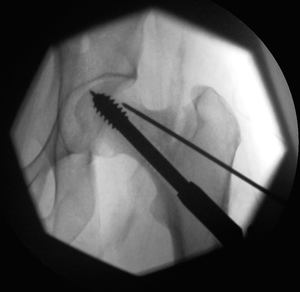
Fig. 96:
stress fracture in 12 year old intraoperative imaging

Fig. 97:
stress fracture in 12 year old intraoperative imaging

Fig. 98:
stress fracture in 12 year old postoperative, post-fixation appearances

Fig. 99:
stress fracture in 12 year old postoperative, post-fixation appearances

Fig. 100:
The patient presented with persistent pain 6 months post fracture...

Fig. 101:
The patient presented with persistent pain 6 months post fracture fixation:...

Fig. 106:
Now 15 years of age, postoperative PAO

Fig. 107:
Now 15 years of age, postoperative PAO

Fig. 108:
Now 15 years of age, postoperative PAO

Fig. 109:
Now 15 years of age, postoperative PAO

Fig. 110:
Post traumatic myositis ossificans presenting with impingement: AP pelvis...