ESSR 2017 / P-0319
A case series review: The rarity of acromion tumours
Congress:
ESSR 2017
Poster Number:
P-0319
Type:
Educational Poster
Keywords:
Pathology, Metastases, Cancer, Education, Ultrasound, MR, CT, Musculoskeletal system, Musculoskeletal bone, Anatomy
Authors:
K. Paramesparan1, A. Shah1, A. M. Davies2, S. L. James2, R. Botchu2; 1Leicester/UK, 2Birmingham/UK
DOI:
10.1594/essr2017/P-0319

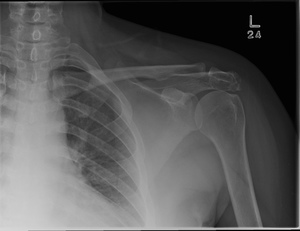
Fig. 1:
Left shoulder radiograph demonstrating a destructive lytic lesion with...

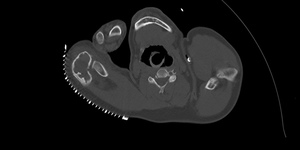
Fig. 2:
Axial CT slices demonstrating a destructive lytic lesion with scalloping of the...

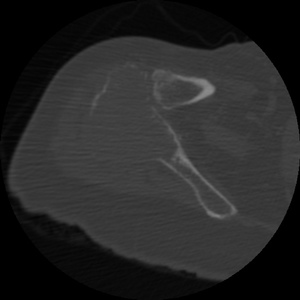
Fig. 3:
Sagittal CT slice demonstrating a destructive lytic lesion with scalloping of...

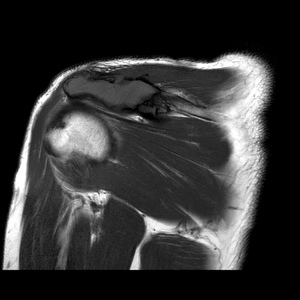
Fig. 4:
T1W Axial MRI demonstrating an isointense to skeletal muscle lesion in the...

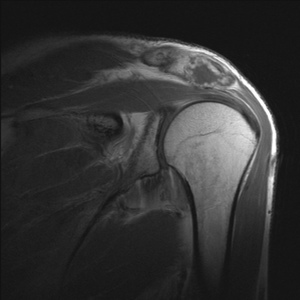
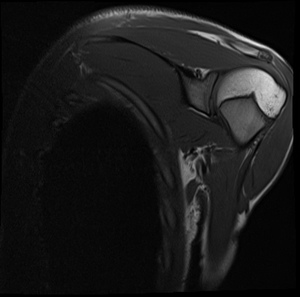
Fig. 5:
Fluid sensitive MRI of the acromion chondrosarcoma with variable inhomogeneity...

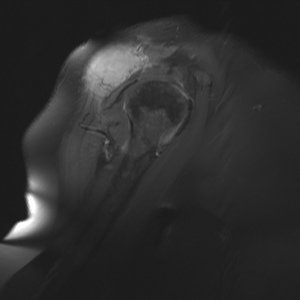
Fig. 6:
Post contrast T1 FS coronal image of the chondrosarcoma demonstrating a...

Fig. 7:
Radiograph of the right shoulder demonstrating a destructive and sclerotic bone...

Fig. 8:
Volume rendered CT demonstrating the sclerotic lesion in the acromion process...

Fig. 9:
T1W axial MRI demonstrating a destructive low signal intensity lesion in the...

Fig. 10:
Fluid sensitive MRI demonstrating increased signal within the acromion lesion...

Fig. 11:
T2W sagittal MRI demonstrating no significant fluid signal in the destructive...

Fig. 12:
Right shoulder radiograph of a patient with renal cell carcinoma demonstrating...

Fig. 13:
Axial CT of same patient in Fig. 12 demonstrating an expansile poorly...

Fig. 14:
Right shoulder radiograph demonstrating a subtle lytic lesion within the...

Fig. 15:
Axial CT of a patient with multiple myeloma demonstrating a large soft tissue...

Fig. 16:
T1W sagittal shoulder MRI in a patient with multiple myeloma with an acromion...

Fig. 17:
T2W MRI of the shoulder in the same multiple myeloma patient as Fig 16,...

Fig. 18:
T1W FS axial MRI of the shoulder in the same multiple myeloma patient as Fig...

Fig. 19:
Sagittal MRI post Gadolinium demonstrating contrast enhancement in the acromion...

Fig. 20:
Left shoulder radiograph demonstrating a lytic lesion within the acromion....

Fig. 21:
Axial CT slice demonstrating an expansile soft tissue mass with evidence of a...

Fig. 22:
STIR sagittal shoulder MRI demonstrating high signal intensity within the...

Fig. 23:
T1W coronal slice of the left shoulder demonstrating a low signal intensity ...

Fig. 24:
T2W sagittal slice of the left shoulder demonstrating a low signal intensity...

Fig. 25:
Post contrast coronal MRI imaging of the left shoulder demonstrating homogenous...

Fig. 26:
T1W coronal MRI of the right shoulder demonstrating a low to intermediate...