Ultrasound findings can help us diagnose soft tissue lesions mainly by their appearance (cystic,
solid…),
histologic origin (epidermic,
dermic,
hypodermic),
anatomic localization and vascularization.
Epidermic inclusion cysts:
Hypoechoic cysts )posterior acoustic enhancement) connected to dermis,
they can show a subepidermic track
Can be heterogeneous (if infected or chronic) or with lobulated/irregular margins with surrounding foreign body reaction (because of keratin leak if it breaks)

Fig. 2: Epidermic inclusion cyst
Trichilemal cyst:
Heterogeneous cysts (posterior acoustic enhancement) with hyperechoic lines and calcification.
They appear in the head.
It may not connect with the dermis (differential with epidermal inclusion cyst)

Fig. 3: Trichilemal cyst
Pilonidal cyst
Lesion arising in the dermis of the intergluteal cleft.
With hyperechoic lines (of pilous material).
Can lead to abscesses

Fig. 4: Pilonidal cyst
Hidradenitis suppurativa:
Dermis thickening in axillary,
inguinal or perineal regions
Can lead to abscesses

Fig. 5: Hidradenitis suppurativa
Vascular malformations:
Hypervascular (arterial or venous specter) or with lack of flow (in lymphatic malformations)

Fig. 6: High flow vascular malformation
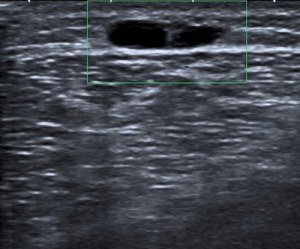
Fig. 7: Lack of Doppler signal in a lymphangioma
Venous malformations can show flebolites
Lipoma:
Hyper or Hypoechoic with hyperechoic lines parallel to the skin
Malignancy must be ruled out in deep (intramuscular) tumors and lesions with atypical findings (over 10 cm,
rapid growth,
non-lipomatous components,
high vascularity or fascial infiltration)

Fig. 8: Typical lipoma

Fig. 9: Atypical lipoma with non-lipomatous component and high vascularization

Fig. 10: Atypical lipoma with non-llipomatous components. Pathology: liposarcoma with fibroid and myxoid components

Fig. 11: Deep intradeltoid lipoma
Fat necrosis:
Very variable appearance from hyper with hypoechogenic areas to hypoechoic lobulated lesions.
They can calcify

Fig. 12: Fat necrosis

Fig. 13: Fat necrosis
Neurofibroma:
Peripheral nerve benign tumor.
It can also appear in the dermis.
Commonly there’s hyperpigmentation of overlying skin
Multiple in NF type I

Fig. 14: Neurofibromatosis type I
Schwannoma:
Oval-shaped,
can show cystic areas and calcifications

Fig. 15: Schwannoma with continuity with the superfificial branch of the radial nerve
Fibromatosis:
May be hypervascular and ill-defined with infiltrative margins (infiltrative growth)
May be superficial (palmar and plantar fibromatosis,
usually small and slow growing) or deep (desmoid tumor,
usually bigger and growing faster)

Fig. 16: Dupuytren (palmar fibromatosis) infiltrating the 4th finger flexor sheath

Fig. 17: Irregular margins and vascularization in desmoid tumor
Foreign body granulomatosis:
After surgery,
trauma of inyections
Hyperechoic foreign body with hyopechoic halo (inflammatory reaction)

Fig. 18: Hipoechoic granulomatosis secondary to hiperechoic lineal foreign body
Rheumatoid nodules:
Solid hypoechoic nodules adjacent to tendons.
Most commonly over olecranon and Achilles tendon

Malignant lesions:
May appear as benign lesions,
but some findings that should raise concern for malignancy are:
-Fast growing painless mass
-Irregular margins
-Necrotic areas
-Hypervascularity
-Pseudopaniculitis can be the appearance of skin lymphomas or leukemia cutis

Fig. 19: Rheumatoid nodule over Achilles tendon

Fig. 20: Lymphadenopathy in diffuse large B-cell lymphoma: Irregular margins

Fig. 21: Lymphadenopathy in follicular B-cell lymphoma: Necrotic area and hypervascularization

Fig. 22: Myxofibrosarcoma: Lobulated fast-growing painless mass with vascularity

Fig. 23: Painless pseudopaniculitis should raise concern for skin lymphoma or leukemia cutis
