ESSR 2018 / P-0090
5th metatarsal bone: let’s freshen up! Anatomy and pathology from pediatric to adult age
Congress:
ESSR 2018
Poster Number:
P-0090
Type:
Educational Poster
Keywords:
Trauma, Education and training, Education, MR, CT, Conventional radiography, Musculoskeletal system, Musculoskeletal bone
Authors:
N. Romano1, F. Sertorio1, M. Marino2, I. Mussetto3, A. Fischetti1, J. P. Zawaideh1, A. Muda1, G. M. Magnano3; 1Genova/IT, 2Roma/IT, 3GENOA/IT
DOI:
10.1594/essr2018/P-0090

Fig. 2:
X-ray: 1 y.o. child

Fig. 3:
X-ray: 3 y.o. child

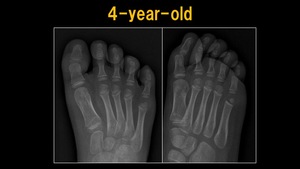
Fig. 4:
X-ray: 4 y.o. child

Fig. 5:
X-ray: 6 y.o. child

Fig. 6:
X-ray: 7 y.o. child

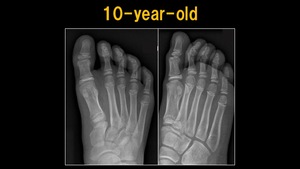
Fig. 7:
X-ray: 10 y.o. child

Fig. 8:
X-ray: 12 y.o. child

Fig. 9:
X-ray: 13 y.o. child

Fig. 10:
X-ray: 14 y.o. child

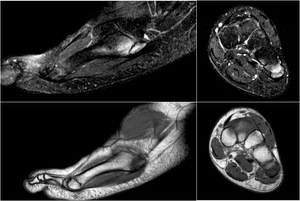
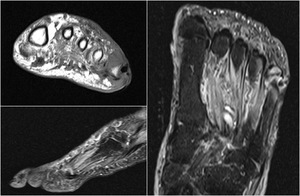
Fig. 11:
MRI: Iselin Disease

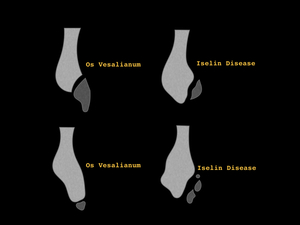
Fig. 12:
Differential diagnosis between Iselin Disease and Os Vesalianum

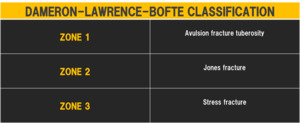
Fig. 13:
Dameron-Lawrence-Bofte classification

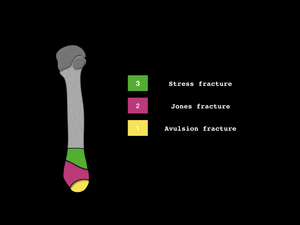
Fig. 14:
Drawing of Dameron-Lawrence-Bofte classification

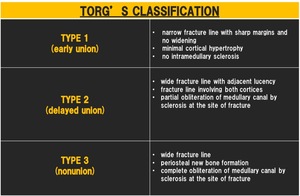
Fig. 15:
Torg's classification

Fig. 16:
X-ray: Zone 1 fracture

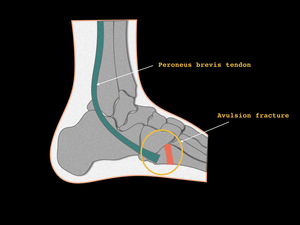
Fig. 17:
Drawing of avulsion fracture

Fig. 18:
X ray: Zone 2 fracture

Fig. 19:
X-ray: zone 3 fracture

Fig. 20:
MRI-diabetic foot: osteomyelitis of the 5th metatarsal bone

Fig. 21:
X-ray: sesamoids of the 5th metatarsal bone