Study patients
Twenty-two patients with diabetic foot underwent MRI to diagnose osteomyelitis and/or CN,
18 with infected ulcer (7 with CN) and 4 with CN without infection (15 man and 7 woman,
mean age 56.59 years,
range age 39-82 years).
The institutional review board at our institution approved the study and written informed consent was obtained in all patients.
Demography and clinical data in Figure 4.
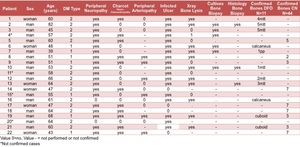
Fig. 4: Demography and clinical data.
MRI protocol
MRI studies were performed in a 1.5T scanner (AERA,
Siemens) with a CP extremity coil,
and routine images in two perpendicular planes to the skin ulcer on T1-weighted SE,
T2-weighted FSE with fat suppression,
and T1-weighted SE with fat suppression before and after contrast were acquired.
For DCE-MRI examinations axial fat-saturated three-dimensional volumetric interpolated breath-hold examination (VIBE) sequence was applied (Table 2),
and after the acquisition of series of flip angles 5º and 10º to obtain T1 mapping,
a bolus injection of 0.1mmol gadobutrol (Gadovist; Bayer,
Berlin,
Germany) per kilogram of body weight and a 20-mL saline flush at a rate of 2.0 mL/s were administered using an automatic power injector.
MRI acquisition protocol in Figure 5.
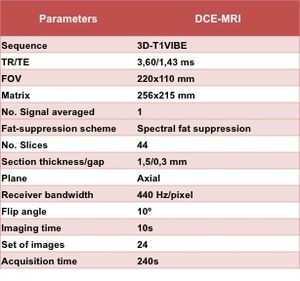
Fig. 5: DCE-MRI acquisition protocol
Bones and DCE-MRI analysis
Bones with DFO were determined by bone biopsy or if on radiographs there was a lytic lesion adjacent to the soft-tissue infection with positive cultures; and bones with CN were defined when morphological MRI revealed a typically subchondral bone oedema with non-infected adjacent soft-tissue.
Finally,
55 bones with proven criteria of osteomyelitis (n=11) and CN (n=44) were evaluated ((11 man and 7 woman,
mean age 56.06 years,
range age 39-82 years).
Demography and clinical data in Figure 4.
Fig. 4: Demography and clinical data.
Two regions of interest (ROIs) of different size (small and covering the whole signal change) were manually sampled independently by two radiologist blinded to the final diagnosis,
in the DCE-MR images in bones with signal changes.
Pharmacokinetic modelling of DCE-MR perfusion was obtained with the Tofts model using a commercial software in a workstation (syngo.MR Tissue4D,
Siemens),
with intermediate population-averaged arterial input function (AIF) and motion correction.
Pharmacokinetic parameters with the Tofts model (Ktrans,
Kep,
Ve),
iAUC and TIC were obtained in each bone.
Statistical study
We analysed the accuracy and comparison of the DCE-MR parameters to establish differences between DFO and CN (χ2 and nonparametric tests),
we studied the optimal cut-off values for differentiate DFO (ROC analysis) and the inter-rater reliability (ICC and kappa index),
considering the two sizes of ROIs of the two readers.
The statistical significance value was set at P < 0.05.


