Bones
Ossicles
Accessory ossicles are secondary ossification centres.
These are well-corticated and occur at typical locations.
These are congenital,
although post-traumatic changes and degeneration can mimic the accessory ossicles.
Occasionally,
these can also be confused with fractures [1].
Os Naviculare
This is also known as accessory navicular bones or os tibiale externum.
This is present medial to the navicular bone,
in which the tibialis posterior tendon has a broad attachment with.
It is present in 10% of the population,
and is usually bilateral.
Os naviculare is classified into three different types; Type I being a small sesamoid embedded within the posterior tibialis tendon,
usually asymptomatic; Type II which is larger (range of 1cm),
more triangular in shape,
with cartilagenous connection to the navicular tuberosity; and Type III,
with prominent tuberosity which is also known as cornuate navicular [1].
Type II is the most common,
constituting half of os naviculare,
and tend to be more symptomatic than the other two subtypes,
by way of enthesitis and traction apophysitis.
It usually presents as median foot pain aggravated by activity.
Fig. 1

Fig. 1: Coronal STIR foot demonstrating Type II os naviculare with oedema-like marrow signal
References: Chelsea and Westminster Hospital, UK
Type III os can be symptomatic as a result of the bony protuberance.
Fig. 2

Fig. 2: Type III or cornuate navicular
References: Chelsea and Westminster Hospital, UK
Os Acromiale
This represents unfused accessory ossification centres of the acromion process.
The shape depends on the fusion pattern of the acromial ossification centres,
of which the meta/meso-acromional subtypes are the most common.
This can be seen in 8% of the population and is usually bilateral.
These are diagnosed above the age of 25,
an age cut-off when the secondary ossification centres are expected to have fused with the acromion process.
Whilst these are usually asymptomatic,
there is a risk of shoulder impingement and rotator arthropathy due to increased mobility of the ossicle [2].
Fig. 3
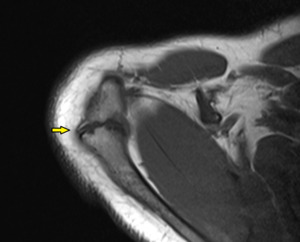
Fig. 3: Type A os acromiale, arises from failure of fusion of the meso-acromion and meta-acromion.
References: Chelsea and Westminster Hospital, UK
Bipartitie medial cuneiform
Arises from two ossification centres of the medial cuneiform.
The combined size of the medial cuneiforms is larger than a conventional cuneiform.
The reported incidence is less than 1%,
more common in males.
These can be associated with additional foot and ankle accessory ossicles,
carpal coalition,
and spinal segmentation anomalies.
If symptomatic,
pain is usually the main complain [3] [4].
Fig. 4

Fig. 4: Bipartitie medial cuneiform
References: Chelsea and Westminster Hospital, UK

Coalition
Coalition refers to the fusion of two or more carpal or tarsal bones.
This can be bony,
fibrous or cartilaginous.
There is a 2% prevalence of carpal coalition in the population whereas tarsal coalition has a prevalence of 5% [5].
In the carpal bones,
the most common coalitions are carpitohamate and lunotriquetral Fig. 6 .
Coalition has been associated with different syndromes such as Turner or Holt-Oram syndrome.
The majority of tarsal coalitions are calcaneonavicular and talocalcaneal,
accounting for 90% of all tarsal coalitions [6].
These can be associated with pes palnus or pain.

Nerve
Median nerve
There are various anatomical variations involving the median nerve.
Bifid median nerve
The median nerve typically courses the carpal tunnel as a single nerve.
In 1-3% of the population undergoing carpal tunnel release,
there is proximal or high bifurcation in which the median nerve divides into the muscular (or recurrent branch) and the sensory component proximal to the transverse carpal ligament [7].
This is also known as bifid median nerve and can be associated with a persistent median artery.
This bifid variant is implicated with carpal tunnel syndrome.
In addition,
the persistent median artery usually has a superficial course and can be inadvertently injured during carpal tunnel release [7].
Fig. 7
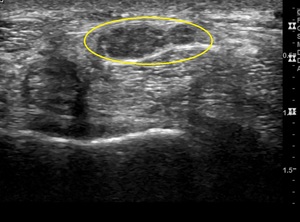
Fig. 7: Transverse view of median nerve deep to the transverse carpal ligament, demonstrating bifid median nerve configuration (circled).
References: Chelsea and Westminster Hospital, UK

Anomalous course of median nerve
The median nerve is usually located at the superficial aspect of the carpal tunnel,
just deep to the transverse carpal ligament.
We demonstrate two cases of carpal tunnel syndrome,
where the site of median nerve impingement is likely to relate to the course of the median nerve,
where it descends dorsally to lie deep in the tunnel,
nestled between the flexor pollicis longus and flexor digitorium profundus of the index finger.
The median nerve is swollen at this site and in both cases,
the findings are supported by EMG studies. Fig. 8 Fig. 9 
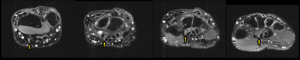
Fig. 8: Axial fluid-sensitive sequences obtained from proximal to distal wrist.
The median nerve (arrow) takes an anomalous course, descending between the flexor pollicis longus and flexor digitorium profundus of the index finger to lie deep within the carpal tunnel. Associated swelling of the median nerve indicating impingement which is also confirmed on nerve conduction studies.
References: Chelsea and Westminster Hospital, UK
Supracondylar Bone Spur/ Ligament of Struthers
There is a bone spur that arises from the volar and ulnar aspect of the distal humerus oriented towards the elbow joint,
which is seen in 3% of the population [8].
Struther’s ligament is the connective tissue that arises from here and attach at the median humeral condyle which can impinge on the median nerve or brachial artery as the neurovascular bundle passes under it.
Fig. 10 

Fig. 10: Supracondylar or avian spur
References: Chelsea and Westminster Hospital, UK
Sciatic nerve
The sciatic nerve is formed by L4-S3 nerve roots and is the largest motor and sensory nerve in the body,
providing most of the sensory innervation to the lower limb.
After forming anterior to the piriformis muscle,
it exits the pelvis inferior to the piriformis through the greater sciatic foramen.
In 16% of assumed normal population,
it may pass through the piriformis muscle instead of beneath it [9] [10].
There is controversy around this variant as a cause for piriformis syndrome which in itself,
is also a controversial entity [9].
Symptoms described are that of buttock and posterior sciatica that is reproduced on internal rotation and adduction of a flexed hip.
Fig. 11
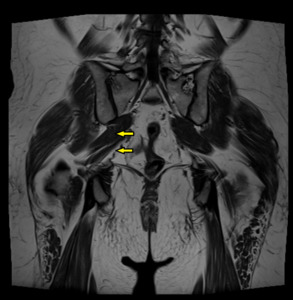
Fig. 11: T1 coronal pelvis. The right sciatic nerve exits the pelvis between the piriformis muscle (arrowed).
Conventional pathway of sciatic nerve demonstrated on the left, exiting inferior to the piriformis
References: Chelsea and Westminster Hospital, UK

Muscles and Tendons
Low-lying Flexor Digitorium Superficialis
The carpal tunnel is an enclosed space which is formed by the transverse carpal ligament and the carpal bones.
It contains the eight flexor tendons of the 2-5th digits,
the flexor pollicis longus as well as the median nerve.
Occasionally,
low-lying muscle fibers from the flexor digitorium superficialis can be seen within the carpal tunnel which may in turn,
result in carpal tunnel syndrome due to its mass effect. Fig. 12
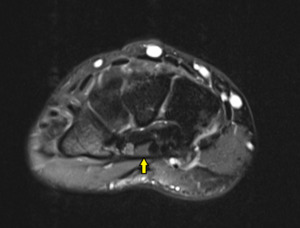
Fig. 12: Low-lying flexor digitorium superficialis slip
References: Chelsea and Westminster Hospital, UK
Accessory muscles
There are numerous accessory muscles found in different parts of the body.
This may be in the way of additional muscles,
heads,
or alteration in course,
attachment or insertions.
These are usually asymptomatic and incidental although depending on their locations,
they may result in pain,
compartment syndrome or neuropathy.
One must be wary to not mistake these as soft tissue tumours.
A few common accessory muscles are as described.
Anconeus epitrochlearis
This muscle extends from the medial cortex of the olecranon and insert at the inferior surface of the medial epicondyle.
When present,
it forms the roof of the cubital tunnel [11].
Fig. 13
The muscle has a reported prevalence of 11% in surgical papers and can commonly be bilateral [12].
This muscle can be associated with cubital tunnel syndrome from compression of the ulnar nerve,
given the proximity and spatial relationship to the ulnar nerve as it traverses the cubital tunnel.
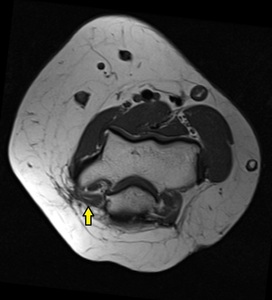
Fig. 13: Anconeus epitrochearis forming the roof of the cubital tunnel
References: Chelsea and Westminster Hospital, UK

Extensor carpi radialis intermedius (ECRI) and other ECU2 variants
ECRI arises from the extensor carpi radialis brevie (ECRB) and courses between the extensor carpi radialis longus (ECRL) and ECRB in the second extensor compartment.
It inserts in the base of the second or third metacarpal.
This can be observed in 12-24% of the population.
Whilst this is usually asymptomatic,
it is important to not mistake this for pathology,
or tendon split.
It has been described in the literature,
as a suitable harvest for tendon transfers [11].
Fig. 14
Other variations exists in this compartment include accessory ECR brevis arising medial to the normal ECRB,
with its own anomalous muscle belly,
and split insertion of the ECRB.
It is important to distinguish these from ECRB longitudinal split tear [11].
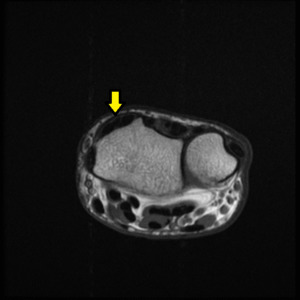
Fig. 14: Extensor carpi radialis intermedius
References: Chelsea and Westminster Hospital, UK

Gastrocnemius slip
Gastrocnemius normally has two heads; medial and lateral.
Accessory slips may occur from either head,
with an estimated frequency of 5%.
In young patients presenting with calf claudication,
the prevalence may be up to 21% [11].
This variant may cause popliteal artery entrapment syndrome from compression of the popliteal neurovascular bundle.
The accessory slip from the lateral head is usually more implicated in this.
Arteries are usually affected,
although popliteal vein involvement has also been described.
The patients are usually young,
athletic,
and typically present with intermittent calf claudication. [13].
Fig. 15

Fig. 15: Lateral gastrocnemius accessory slip
References: Chelsea and Westminster Hospital, UK
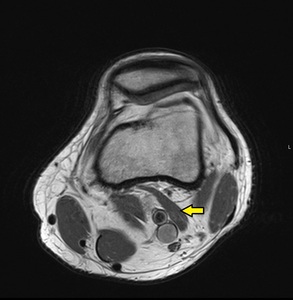
Fig. 16: Lateral gastrocnemius accessory slip
References: Chelsea and Westminster Hospital, UK
With dynamic imaging,
normal arterial lumen may be demonstrated to narrow in stress maneuvers.
This may be useful in assessing significance,
and severity of the compression [13].
Fig. 17
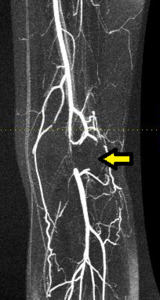
Fig. 17: MR-angiogram of the same patient demonstrating short segment occlusion of the popliteal artery secondary to the accessory gastrocnemius slip
References: Chelsea and Westminster Hospital, UK

Accessory flexor digitorium longus
The accessory FDL can be seen in 2-8% of the population.
It courses posteromedial to the FHL at the level of the tarsal tunnel and inserts into the quadratus plantae or flexor digitorium longus muscle.
This remains muscular in the tarsal tunnel,
and hence should not be mistaken for a FHL accessory tendon slip.
It also lies deep to the flexor retinaculum,
which helps differentiate it from accessory soleus muscle.
Its course in the tarsal tunnel can predispose to tarsal tunnel syndrome [11] [14].
Fig. 18
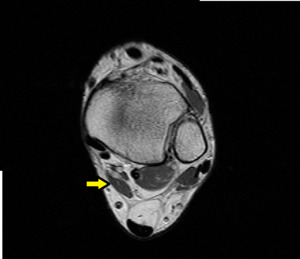
Fig. 18: Accessory flexor digitorium longus
References: Chelsea and Westminster Hospital, UK


Fig. 19: Accessory flexor digitorium longus
References: Chelsea and Westminster Hospital, UK
Peroneus Quartus
Multiple accessory peroneal muscles have been described,
including peroneus accesorius,
peronocalcaneus externum and peroneus quartus muscles,
with varied overlapping classification and descriptive terminology,
resulting in confusion in the literature.
Hence,
peroneus quartus is collectively used to describe the accessory peroneal muscles in the lateral compartment [11].
The peroneus quartus originates from the distal lateral fibula or the peroneal muscles,
and can have insertions in the calcaneus,
cuboid or peroneus longus tendon.
The most common distal attachment is the retroctochlear eminence of the calcaneus.
Together with the peroneus brevis and longus,
it stabilizes hind-foot pronation and everts the ankle.
The prevalence varies in the literature,
from 10-30%.
Fig. 20
It may present with lateral ankle pain from tenosynovitis and tendinopathy,
as well as instability and subluxation as the additional mass effect in the lateral compartment can predispose to chronic mechanical attrition [15].
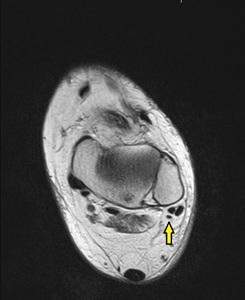
Fig. 20: Peroneus quartus
References: Chelsea and Westminster Hospital, UK

Peroneus Tertius
Despite its name,
the peroneus tertius is located in the extensor compartment,
not the peroneal or lateral compartment.
As such,
it is not included in the broad ‘peroneus quartus’ term.
The muscle is located anteriorly,
arising from the anterior surface of the distal fibula,
interosseous membrane and extensor digitorium muscle.
This tendon is commonly encountered in cadaveric studies and may well be considered a norm [11].
The tendon passes deep to the extensor retinaculi and insert onto the base and the dorsal surface of the 5th metatarsal shaft.
It is usually asymptomatic,
although it has been implicated as a cause for snapping sensation over the lateral dome of the talus.
Fig. 21
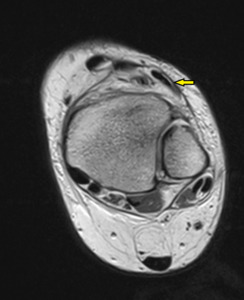
Fig. 21: Peroneus Tertius
References: Chelsea and Westminster Hospital, UK

Accessory soleus
Accessory soleus arises from the posterior aspect of tibia or deep fascia of soleus,
and can be found in 6% of the population [11] [14].
It can insert in the distal Achilles or have muscular or tendinous insertion in the calcaneum.
This can present as swelling,
of which the majority (67%) would be painless.
Fig. 23 Pain may arise from ischemia or posterior tibial nerve compression from extrinsic compression of the tarsal tunnel [15].
The age of presentation is usually in the 20s,
due to the increased size from physical activity.

Fig. 22: Accessory soleus
References: Chelsea and Westminster Hospital, UK
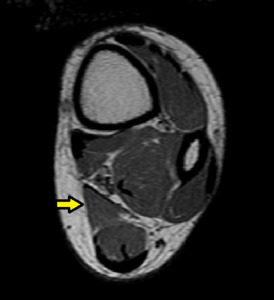
Fig. 23: Accessory soleus
References: Chelsea and Westminster Hospital, UK








. References: Chelsea and Westminster Hospital, UK")


.
Conventional pathway of sciatic nerve demonstrated on the left, exiting inferior to the piriformis References: Chelsea and Westminster Hospital, UK")












 takes an anomalous course, descending between the flexor pollicis longus and flexor digitorium profundus of the index finger to lie deep within the carpal tunnel. Associated swelling of the median nerve indicating impingement which is also confirmed on nerve conduction studies. References: Chelsea and Westminster Hospital, UK")