OSSEOUS ANATOMY
The sacropelvic structural stability is conferred by the sacrum and bilateral innominate bones,
and ligaments that collectively form the pelvic ring's osteo-ligamentous complex [7].
The sacrum is a triangular bone in the lower part of the vertebral column.
It articulates with the last lumbar vertebra (typically L5) and coccyx,
at its base and apex,
respectively.
Laterally,
it articulates with the iliac bones on either side,
forming the sacroiliac joints.
Dorsally,
there are the sacral foramina,
where the anterior and posterior divisions of the sacral nerves exit,
and the lateral sacral arteries enter (Fig.
1) [8].
The two innominate bones (coxal) bones articulate with the sacrum and proximal femora.
Each innominate bone is composed of 3 united bones,
the ilium,
ischium and pubis.
These converge in the acetabular fossa at the triradiate fusion center (Fig.
2).
PATHOPHYSIOLOGY
With advancing age, reduction in bone remodelling capacity and lower hormone levels weaken the bone's internal architecture,
resulting in normal compact bone being converted to immature callus; this makes it susceptible to fractures even with minimal force [9].
In the sacrum,
the ISFs correspond to areas that show significant cancellous bone density reduction and increased stress loads while walking (based on biomechanical models) [10].
SACRAL AND PELVIC ISFs - COMMON SITES
The common locations of sacropelvic ISFs include the iliac wings,
medial iliac margins,
pubic rami, supraacetabular and parasymphyseal regions,
and just lateral to the sacral foramina (Fig.
3).
The knowledge of these common locations can help avoid misinterpretation of imaging findings.
ASSOCIATED INJURIES
ISFs can result in concomitant injuries to the surrounding soft tissue structures i.e.
muscles and tendons causing varying grades of severity from strain,
sprain to complete tears (Fig. 4).
Conversely,
soft tissue injuries can help find osseous pathology,
for example,
if an intramuscular haematoma is present,
the tendon insertion site should be evaluated for presence of a fracture.
IMAGING
Imaging has an important role in detection and diagnosis of ISFs.
Findings vary depending on the type of activity,
site and timing of imaging in relation to injury [11].
Radiographs
Most patients are initially investigated with radiographs of the pelvis and hip,
or lumbosacral spine. While fractures of the anterior pelvic ring such as pubis and ischium are easily identified,
sacral and posterior iliac fractures can be difficult to detect (Fig. 5) as they may be obscured by overlying bowel gas.
Overall,
the sensitivity of radiographs may be as low as 15% depending on the time the radiograph was acquired after the injury [12],
this potentially delaying diagnosis.
Subsequent radiographs performed at delayed presentation may also show variable findings i.e.
lucent fracture line or sclerosis [13].
Further,
the presence of periostitis or new bone formation can mimic malignancy,
resulting in unnecessary biopsies [14].
In radiographically occult ISFs,
cross sectional imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI) can help in detection and localisation.
However,
MRI is preferred to CT as it provides improved diagnostic accuracy [4,
15].
Computed Tomography
CT helps in detection of cortical breaks,
fracture lines disrupting the bony trabeculae,
focal areas of scleroses,
adjacent radiolucent areas representing resorptive bone changes,
and vacuum phenomenon.
It can also identify soft-tissue abnormalities such as muscle swelling and fat-tissue stranding [4] (Fig.
6).
The main disadvantage of CT is patient exposure to ionising radiation. However,
the increasing use of dual-energy CT (DECT) with advanced post-processing techniques allows for material-specific (e.g.
water) images to be generated [16].
This is useful in detection of marrow oedema and help localise fracture.
While DECT can potentially reduce scan time and provide earlier diagnosis,
image quality problems from motion,
patient habitus and metallic artifacts may still arise from time to time [16].
Magnetic Resonance Imaging
MRI is highly sensitive and specific due to its superior marrow visualisation and soft tissue contrast.
Hence,
it can discern other causes of pain (i.e.
distinguish soft tissue,
bone or joint problems).
ISFs typically manifest as linear low signal linear focus within the marrow on T1-weighted images.
On T2-weighted imaging,
the low signal line is surrounded by high T2-weighted area of marrow oedema; this high signal area is interpreted as bone contusion when there is non-visualisation of the fracture [17] (Fig.
7).
Nuclear Medicine Imaging
Bone scintigraphy evaluation with Technetium-99m tracer demonstrates increased activity at the sites of insufficiency fractures.
Diagnostic features of sacral insufficiency fractures are: (i) characteristic "Honda-sign" with vertical fractures through both sacral ala,
and a horizontal fracture line through the mid sacrum at the S2 or S3 level or,
(ii) combination of concomitant sacral and parasymphyseal tracer uptake [18].
PEARLS AND POTENTIAL PITFALLS
Clinical information. A thorough review of the clinical history is important in diagnosis of ISFs.
This allows for imaging diagnosis to be appropriately contextualised.
Satisfaction of search.
An insufficiency fracture in one location should prompt a search for other insufficiency fractures.
A study by Aretxabala et al reported that concomitant sacral insufficiency fractures were found in 78% pubic rami insufficiency fractures [19].
In our institution,
lumbar spine MRI is a commonly performed study for chronic low back pain and insufficiency fractures may be partly imaged and go undetected by the radiologist.
Undisplaced fractures. Fracture detection on radiographs may be difficult even though patients that are symptomatic. In older patients,
the presence of osteoporosis makes detection more challenging. Such cases will benefit with cross sectional imaging and require a high index of clinical suspicion for referral.
Proximal femoral fractures.
Insufficiency fractures of the proximal femora such as subchondral femoral head,
femoral neck,
inter-trochanteric and bisphonate-related femoral shaft fractures,
may be the cause of the patient's symptoms.
Care must be taken when reviewing the radiographs to prevent misdiagnosis.
Marrow abnormalities. Potential pitfalls in MRI include failure to recognise and wrong interpretation of marrow morphological and signal changes. An example is ISFs is the failure to recognise an underlying marrow lesion.
Clues to this diagnosis include patient's history,
atypical fracture pattern or radiographic findings.
On MRI,
pathological entities demonstrate low signal (relative to skeletal muscle) area of marrow replacement and expansion on T1-weighted images,
and associated soft tissue component.
Conversely,
radiologists who are unfamiliar with imaging features of insufficiency fractures especially in patients with underlying malignancy may misinterpret findings as osseous metastases [4].
Post-operative insufficiency fractures.
A high index of suspicion for insufficiency fractures is required in patients with recent or prior hip surgery such as total hip arthroplasty (THA), especially in those with osteoporosis and patients with atraumatic onset of persistent pain post-operatively [20].
Recognition and early referral for radiographs or CT can help early diagnosis and prevent undesirable complications.
Mimics of Insufficiency fractures. Other traumatic and non-traumatic conditions can mimic insufficiency fractures,
and can be localised by anatomical location i.e.
bone,
soft tissues,
articular,
periarticular.
Examples include avulsion fractures (bone),
severe degenerative or infectious arthritis (articular),
and myositis ossificans (soft tissue). These entities may co-exist with ISFs.
Hence,
the knowledge of their imaging features entities can help distinguish them from one another.
This helps in prompt patient diagnosis and management.
CASE REVIEWS
Case 1: An 86 year-old female patient with prior right neck of femur fracture treated with right hip bipolar hemiarthroplasty presented for chronic lower back pain and right gluteal pain after blunt low-energy trauma to the right buttock region.
Her clinicians suspect lumbar vertebral insufficiency fracture and ordered a lumbar spine MRI.
The study showed no vertebral fracture.
However, the axial images at the L5 level showed enlargement of the right psoas muscle and break in the anterior cortex of right ilium which were not detected by the reporting radiologist (Fig. 8).
A pelvic MRI and CT performed several days later due to persistent pain showed a comminuted fracture of the right iliac wing (Fig. 9).
This case highlights the importance of review areas and utilising the history given by the clinicians to guide diagnosis.
Case 2: An 85 year-old female patient,
with prior lumbar spine fusion surgery (more than 10years ago) and cervical cancer treated with radical hysterectomy and brachytherapy (3 years ago),
presented for sudden onset right hip pain with sciatica symptoms.
She was able to weight bear and does not recall a recent history of trauma. Given the prior history,
her clinicians suspected osseous metastases.
Apart from an old left parasymphyseal fracture complicated by non-union,
the plain pelvic radiograph was fairly unremarkable.
An MRI performed one day later showed multiple insufficiency fractures at characteristic sites. Bilateral femoral subcapital and L5 vertebra insufficiency fractures were also present.
These were attributed to either osteoporosis or radiation-mediated (Fig.
10). This case highlight difficulties in identification of fractures that are undisplaced and having a high index of suspicion for further imaging.

Fig. 10: Above: Pelvic radiograph showed prior lumbar instrumentation and old left parasymphyseal fracture with malunion. No new displaced fracture was seen. Below: Coronal inversion-recovery sequences demonstrated multiple insufficiency fractures involving bilateral femoral subcapital regions (red arrows), L5 vertebral body (yellow arrow), both iliac wings and sacrum (white arrows).
Case 3: A 53 year-old female presented with right hip pain for 1 week duration.
She is on long term bisphosphonate therapy.
Pelvic radiograph was reported as normal.
However,
the characteristic cortical beak appearance of the lateral cortex of the proximal femur was not identified and described.
Repeat radiograph performed 2 weeks later showed a displaced proximal femoral fracture (Fig.
11).
This case highlights the importance to scrutinize the proximal femora for abnormalities especially if there is known relevant history such as in this case.

Fig. 11: Pelvic radiographs performed 2 weeks apart for 53 year old patient on long term bisphosphonate therapy who presented with with right hip pain. Left: Characteristic lateral cortical beak appearance (red arrow) was not reported. Right: Patient sustained a displaced right proximal femoral fracture 2 weeks later.
Case 4: An 84 year-old lady with prior right hip hemiarthroplasty presented with atraumatic persistent right hip pain of 1 week in duration.
Initial pelvic radiograph was unremarkable except for non-specific faint iliac wing sclerosis which was not reported by the radiologist.
Subsequent CT and MRI confirmed presence of fractures but these were initially misinterpreted as pathological entity,
despite PET-CT demonstrating minimal tracer uptake.
Patient underwent further neoplatic work-up which showed no malignancy (Fig.
12).
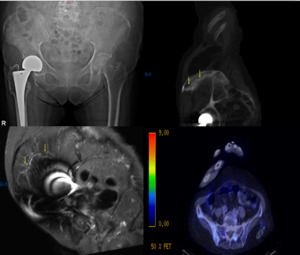
Fig. 12: Above - LEFT : Pelvic radiograph showed prior right hemiarthroplasty, but otherwise normal. CT and MRI showed linear sclerotic (Above - RIGHT) and low signal (Below - LEFT) curvilinear lines parallel to the iliac crest in consistent with insufficiency fracture. However, they were misinterpreted as pathological fractures. PET-CT (Below - RIGHT) showed minimal metabolic activity.
Case 5: An 82 year-old-gentleman,
with history of non-metastatic prostate carcinoma,
presented with chronic atraumatic right hip pain.
Radiograph showed sclerotic foci which were misinterpreted as prostatic bone metastases.
Despite low serum prostate-specific antigen (PSA) levels,
his Technecium-99m bone scintigraphy,
CT and MRI imaging studies were interpreted as osseous metastases.
Patient was given radiation treatment to the right hip and hemipelvis.
Subsequent follow-up CT study showed fracture healing and new intertrochanteric fracture,
attributed to radiotherapy.
He was managed surgically with right hip hemiarthroplasty (Fig.
13).
This case highlights failure to recognise imaging features of ISFs resulting in undesirable patient outcome.
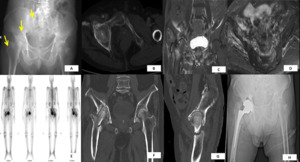
Fig. 13: A: Radiograph showed sclerotic foci (yellow arrows) which were misinterpreted as prostatic bone metastases. B: CT showed sclerosis and lucent fractures in the right supraacetabular region and adjacent superior right pubic ramus. C & D: MRI demonstrated multiple foci of insufficiency fractures characterised by low signal lines surrounded by marrow oedema. E: Bone scintigraphy confirmed the multiplicity of these fractures. However, they were interpreted as metastases despite low baseline post-treatment serum prostate-specific antigen (PSA) levels. F & G: Follow-up CT after radiotherapy showed healing of the insufficiency fractures but development of new right femoral intertrochanteric fracture which was attributed to treatment. H: Post right hip hemiarthroplasty pelvic radiograph.
Case 6: A 28 year-old female patient with chronic myeloid leukemia (CML) presented with bilateral gluteal pain which is more significant on the right,
lasting several days.
Radiographs were normal.
MR Imaging findings demonstrated multiple scattered bone infarcts which were attributed to her underlying medical condition.
However,
there is also a right iliac wing insufficiency (pathological) undisplaced fracture that was missed by the radiologist and showed surrounding gluteal and iliacus muscle oedema (Fig.
14).
This is a difficult case demonstrating concimitant pathologies co-existing with ISFs which may be missed if not carefully evaluated.
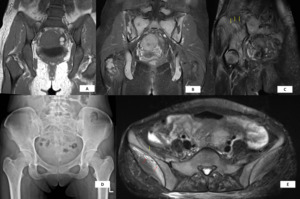
Fig. 14: A: T1-weighted MRI showed diffuse marrow replacement. Incidental fat-containing left adnexal entities are also seen. B: Post- Gadovist (Gadobutrol) T1-weighted fat-saturation image showed multiple foci of intra-medullary bone infarcts attributed to her underlying disease process and treatment. C: Coronal-oblique T2-weighted image showing a low signal undisplaced right iliac wing insufficiency (pathological) fracture (yellow arrows). D: Pelvic radiograph performed one day prior was occult for both fracture and infarcts. E: Axial T2-weighted image showed break in the anterior cortex of the right iliac wing (yellow arrows) with adjacent gluteus maximus and iliacus muscle oedema (red arrows).
Case 7a: 84 year-old female patient with history of liposarcoma of the left lower limb treated with resection more than 20 years prior presented with atraumatic left gluteal pain worsening gradually over several months.
She reports pain on sitting and walking.
Radiograph was normal.
MRI showed a large lobulated peripherally enhancing thick-wall collection with multiple interna septa at the characteristic location of the left ischiogluteal bursa consistent with bursitis (Fig.
15). Patient opted for surgical management.
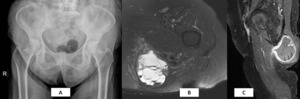
Fig. 15: 84 year-old female patient with history of liposarcoma post-resection presented with atraumatic left gluteal pain worsening gradually over several months. A: Pelvic radiograph was normal. Axial TIRM (B) and post-gadobutrol sagittal T1-weighted fat saturation (C) MR images showed a large lobulated peripherally enhancing thick-wall collection with multiple interna septa at the characteristic location of the left ischiogluteal bursa consistent with ischiogluteal bursitis.
Case 7b: The same patient above sustained a displaced left proximal femoral inter-trochanteric fracture 2 years later which was treated surgically.
She complained of persistent post-surgical medial proximal thigh pain and swelling about 5 months after surgery.
Post-operative pelvic radiograph performed showed no insufficiency fracture but there was soft tissue calcification along the medial thigh distal to the displaced lesser trochanteric osseous fragment which is consistent with myositis ossificans (Fig.
16).

Fig. 16: The same patient in Fig. 15 sustained a displaced left proximal femoral inter-trochanteric fracture two years later and was surgically treated. She complained of persistent post-surgical left medial proximal thigh pain and swelling about 5 months after surgery. Pre-operative (Left) and Post-operative (Right) pelvic radiographs showed no post-surgical insufficiency fractures but there was new soft tissue calcification along the medial-proximal thigh, distal to the displaced lesser trochanteric osseous fragment, consistent with myositis ossificans.

, sacral foramina (yellow arrows) and sacroiliac joints (white arrows).")
, ischium (blue) and pubis (red); these make up the innominate bone. They converge at the triradiate fusion center of the acetabular fossa (black star).")
. In Radiopaedia: Diagram - pelvic insufficiency fractures. Retrieved May 13, 2018, from https://radiopaedia.org/cases/diagram-pelvic-insufficiency-fractures")
 associated with left inferior pubic ramus fracture (red circle). Below: Right pectineal muscle tear (yellow arrow) with haematoma evidenced by intramuscular susceptibility artifacts (white arrow).")
 demonstrated displaced fractures of the right pubic rami. The sacrum was obscured by bowel. MR imaging (right) performed the next day showed right sacral ala fracture in this T1-weighted coronal image.")
 images in bone (above) and soft tissue (below) windows of a 67 year-old male who sustained low-energy trauma. CT provides superior delineation of right iliac fractures (red arrow). Soft tissue window showed swelling of the right iliacus and gluteal muscles (yellow arrows).")
 shows low-signal curvilinear bilateral undisplaced supraacetabular insufficiency fractures (yellow arrows). Coronal-oblique T2-weighted fat-saturated image (right) shows a right low-signal curvilinear iliac wing insufficiency fracture with surrounding high-signal marrow oedema(red arrows).")
 and break in the anterior cortex of the right ilium (yellow arrow).")
 reformat from CT study of the same patient depicting a "3-dimensional" overview of iliac wing comminuted insufficiency fracture.")