Groin hernias:
1.
Indirect Inguinal hernia
A 50-year-old man presented with rapidly increasing abdominal distension,
abdominal pain,
and with a palpable mass in the groin (Fig 1).
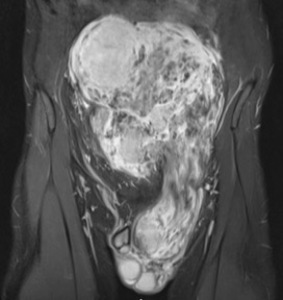
Fig. 1: Coronal fat suppressed T2 weighted image demonstrates a large heterogeneous tumour with internal fat component demonstrating suppression on this fat saturated sequence. The size of the intra-abdominal tumour has resulted in a left indirect inguinal hernia descending through the left inguinal canal to the scrotum. The paucity of fat component and nodularity of the lesion suggested that radiologically this is a high grade, undifferentiated sarcoma and was confirmed on biopsy.
Normal anatomy of the inguinal canal
The inguinal canal in the lower abdominal wall measures approximately 4 cm in length and is lined by the aponeuroses of the three abdominal muscles,
namely the external oblique,
internal oblique,
and transversus abdominis muscles.
The deep and superficial rings are openings at either end of this canal.
The deep ring in the transversalis fascia lies 1cm superior to the inguinal ligament and lateral to the inferior epigastric vessels.
The superficial ring is an opening in the aponeurosis of the external oblique.
Indirect inguinal hernias are the most common type of abdominal wall hernia.
These hernias are located lateral to the inferior epigastric vessels and result from a patent processus vaginalis.
This results in herniation along the spermatic cord into the scrotum in men whilst in women this follows the round ligament into the labia majora [3].
2.
Direct Inguinal hernia
Direct inguinal hernias are often secondary to the weakness of the transversalis fascia.
Contrary to indirect inguinal hernias they are located medial to the inferior epigastric vessels in the posterior wall of the inguinal canal (Hesselbach triangle) [3].
Imaging performed as work up for iron deficiency anaemia in this 60-year-old gentleman detected an incidental intra-pelvic fat containing tumour.
The tumour appears to herniate through a weakness in the abdominal wall as a direct inguinal hernia (Fig 2).
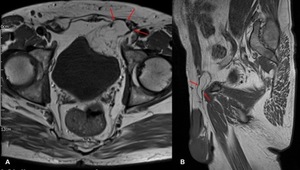
Fig. 2: (A, B) Axial and Sagittal T1 weighted MRI images demonstrates a pelvic tumour of predominantly fat signal intensity which indents the wall of the urinary bladder and extends anteriorly through a defect in the anterior abdominal wall. The hernial sac is medial to the inferior epigastric vessels. The intra-pelvic tumour contains mature fatty elements with imaging characteristics that are indistinguishable from those of normal fat. The numerous septae within the mass however should suggest a diagnosis other than that of a simple lipoma [4].
Ventral hernias:
3.
Spigelian hernia
The linea semilunaris is a fibrous union of the rectus sheath with the aponeuroses of the transverse and oblique abdominal muscles extending from the level of the ninth costal cartilage to the symphysis pubis.
A Spigelian hernia is the result of a defect in the linea semilunaris.
A 40-year-old woman presented with weight loss and left sided abdominal pain.
Cross-sectional imaging revealed an incidental left Spigelian hernia (Fig 3).
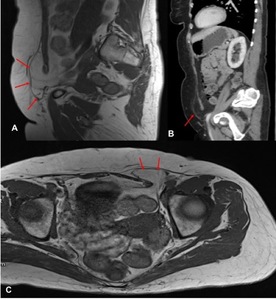
Fig. 3: (A,C) Sagittal and axial T1 weighted MR images demonstrate a left-sided defect in the linea alba. An intra-abdominal tumour is seen to herniate through this defect and is iso-intense to the subcutaneous fat. A few internal septations makes this more than a simple lipomatous tumour. The Spigelian hernia can also be clearly seen on sagittal CT reformats (B). The fat content on CT returns a ‘dirty’ signal however the septations are more clearly delineated on MR.
4.
Divarication of the rectus abdominus
An MRI performed on this 70-year old gentleman for unrelated reasons revealed divarication of the rectus abdominus secondary to a lipomatous lesion (Fig 4).
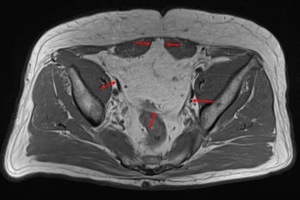
Fig. 4: A weakness in the linea alba results in protrusion of the intra-abdominal fat containing tumour (outlined, red arrows) between the two recti. This T1 weighted axial image demonstrates internal septations and subtle nodularity.
Posterior hernias:
5.
Lumbar hernia
Lumbar hernias occur through defects in the lumbar muscles or the posterior fascia in the superior (Grynfeltt-Lesshaft) or inferior (Petit’s) lumbar triangles.
A third type of lumbar hernia,
the diffuse lumbar hernia is often iatrogenic and may occur following surgical incisions [2].
55-year-old lady presents with lateral abdominal discomfort.
A MRI was performed as this pain was thought to be discogenic in nature.
A left lumbar hernia containing a fat-predominant retroperitoneal mass was picked up incidentally (Fig 5).
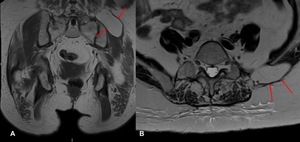
Fig. 5: Coronal and axial T1 weighted MR images demonstrate a defect in left abdominal wall at inferior lumbar triangle, with protrusion of a retroperitoneal tumour with predominant fat signal intensity, into the subcutaneous tissues (red arrows).
A young lady presenting with right sided abdominal pain was found to have a retroperitoneal liposarcoma on subsequent MRI (Fig 6).
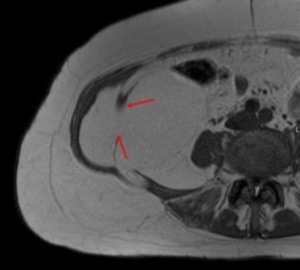
Fig. 6: Axial T1 weighted image of the lower abdomen shows a defect in the right lateral abdominal wall with a defect in the right internal oblique muscle and protrusion of a large biopsy proven liposarcoma into the abdominal wall (red arrows).
Pelvic hernias:
6.
Sciatic hernia
Sciatic hernias are rare hernias.
Cross sectional imaging plays an important role in diagnosing sciatic hernia and MRI is the modality of choice to evaluate the sciatic nerve in cases of sciatic hernia [6].
A 70-year-old lady complained of right sided sciatica.
MRI lumbar spine identified a partially visualised mass and subsequent dedicated MRI pelvis was performed revealing a large sarcomatous mass herniating through the right greater sciatic foramen which was causing secondary compression of the right sciatic nerve (Fig 7).
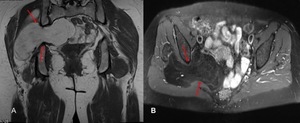
Fig. 7: Coronal T1 weighted MR image, red arrows outline the large intra-pelvic tumour which herniates through the right sciatic foramen. While the tumour returns a fat signal isointense to the subcutaneous fat, internal striations and heterogeneity can be seen in keeping with a high grade sarcoma. (B) Axial STIR image of the pelvis confirms that the lesion is predominantly fat containing as it supresses on fat saturated sequences. High signal septations which do not supress can be visualised.
7.
Iliopsoas
The iliopsoas compartment is composed of the psoas major,
psoas minor,
and iliacus muscles which have a common fascial sheath and fuse to form a common tendinous insertion into the lesser trochanter.
Violation of the retroperitoneal fascial planes by neoplastic processes may give rise to lesions within this compartment and the iliopsoas compartment may act as a conduit for the distant spread of disease [7].
The iliopsoas compartment is a rare site for soft tissue sarcoma [9].
A CT performed for increasing lower abdominal pain in a middle aged lady picked up a large incidental sarcomatous lesion in the right iliopsoas compartment.
This was characterised on a dedicated MRI (Fig 8).
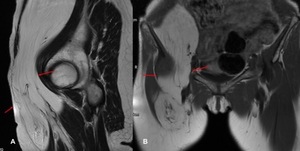
Fig. 8: (A, B) Sagittal and coronal T1 weighted MR images demonstrate a large lipomatous tumour arising from the right iliopsoas compartment (red arrows) extending into the right groin and upper thigh. The size and thick septations points towards a sarcomatous lesion radiologically.
Sarcomas in the iliopsoas compartment have a poorer outcome than those located in other areas,
as the tumour can grow undetected for longer periods of time.
The tumours in this compartment are often surgically inaccessible due to their proximity to vital structures and are often associated with a poor survival [8].


 Axial and Sagittal T1 weighted MRI images demonstrates a pelvic tumour of predominantly fat signal intensity which indents the wall of the urinary bladder and extends anteriorly through a defect in the anterior abdominal wall. The hernial sac is medial to the inferior epigastric vessels. The intra-pelvic tumour contains mature fatty elements with imaging characteristics that are indistinguishable from those of normal fat. The numerous septae within the mass however should suggest a diagnosis other than that of a simple lipoma [4].")
 Sagittal and axial T1 weighted MR images demonstrate a left-sided defect in the linea alba. An intra-abdominal tumour is seen to herniate through this defect and is iso-intense to the subcutaneous fat. A few internal septations makes this more than a simple lipomatous tumour. The Spigelian hernia can also be clearly seen on sagittal CT reformats (B). The fat content on CT returns a ‘dirty’ signal however the septations are more clearly delineated on MR.")
 between the two recti. This T1 weighted axial image demonstrates internal septations and subtle nodularity.")
.")
.")
 Axial STIR image of the pelvis confirms that the lesion is predominantly fat containing as it supresses on fat saturated sequences. High signal septations which do not supress can be visualised.")
 Sagittal and coronal T1 weighted MR images demonstrate a large lipomatous tumour arising from the right iliopsoas compartment (red arrows) extending into the right groin and upper thigh. The size and thick septations points towards a sarcomatous lesion radiologically.")