Conventional radiography
The IPS acts similar to a primary ossification center and its ossification is variable with respect to the rate and pattern of mineralization.
Radiographic changes usually include a well-marginated expansile lesion,
osteopenia,
radiolucencies,
and patchy calcifications,
with a normal structure of the surrounding bone.
It is a common finding at radiologic workup,
with a reported prevalence by Ross and Caffey of about 50% in children 6 to 8 of age,
and 20% in children from 2 to 19 years of age according to Palme (5).
These changes are frequently observed incidentally in asymptomatic patients imaged for other reasons and are usually asymmetric.
This unpredictable appearance should be recognized to avoid unnecessary intervention.
Additionally,
due to its tumor-like appearance,
it may lead to problems in the differential diagnosis of both symptomatic and asymptomatic children

Fig. 1: Fig. 1 - Pelvic radiograph, frog leg lateral view, of a 10-year old girl, showing an expansile lucent lesion in the left ischiopubic synchondrosis, with well-defined borders and no periosteal reaction.

Fig. 2: Pelvic radiograph anteroposterior pelvis view, of a 4-year old girl complaining of groin pain, showing a well-marginated expansile lesion with faint radiolucencies in the left ischiopubic synchondrosis (a), and complete ossification 8 months later (b).
Ultrasound
Although ultrasound is a valuable imaging method in the pediatric population,
its role in the evaluation of Van Neck-Odelberg disease has not been described in the literature.
Computed Tomography:
Computer tomography (CT) offers the advantages of a better depiction of the bone details,
periosteal reaction, and mineralization.
Besides,
it allows reconstructions and three-dimensional reformatting,
which may be valuable in a correct interpretation.
Although cortical bone detail is excellent,
marrow evaluation is limited.
One must always be aware of the increased radiation exposure and that children are considerably more sensitive to radiation than adults.
Therefore CT should be reserved for specific cases,
ideally with low-dose protocols.
As in conventional radiography,
findings at CT include an expansile lucent lesion in the IPS projecting into the obturator foramen,
with well-defined borders.
There is no soft tissue component and no periosteal reaction or significant bone destruction,
suggesting a benign etiology.
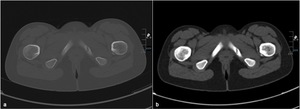
Fig. 3: Axial pelvic CT of a 10-year old girl, bone (a) and soft tissue (b) window, showing an expansile lucent lesion in the left ischiopubic synchondrosis, with well-defined borders and no soft tissue component nor periosteal reaction.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) allows excellent tissue characterization,
is multiplanar and uses no ionizing radiation.
However,
it is costly,
has a relatively long exam time and may require sedation.
MRI can be helpful in the differentiation of IPS from a pathologic condition,
because of its excellent ability of tissue characterization.
Most common features involve signal alteration and contrast enhancement of the bone marrow,
which is hyperintense on fat-suppressed T2-weighted and STIR sequences and hypointense on T1-weighted sequences.
Other findings include swelling of the adjacent soft tissue,
which appears as hyperintense signal alteration on fat-suppressed T2-weighted and STIR sequences.
These findings are indicative of hyperemia edema,
probably due to mechanical stress on this temporary joint.
A more characteristic finding appears to be a band-like hypointense area in the center of the synchondrosis on all sequences,
consistent with fibrosis.
This finding,
as well as the well-defined margins of the ischiopubic bone,
is helpful in ruling out a neoplastic lesion.
This is nevertheless non-specific.
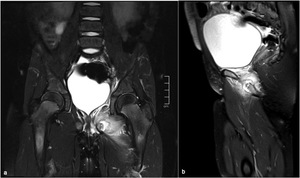
Fig. 4: Pelvic MRI of a 5-year old girl, coronal FS T2WI (a) and sagittal FS DPWI (b), showing bone marrow edema involving the left ischiopubic synchondrosis, with subperiosteal liquid. There is also marked swelling of the adjacent muscles.
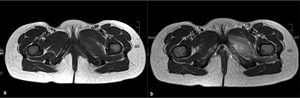
Fig. 5: Pelvic MRI of a 5-year old girl, axial T1 (a) and axial T2W images (b), showing a band-like hypointense area in the center of the left ischiopubic synchondrosis, consistent with fibrosis. One can also see swelling of the adjacent soft tissue as a hyperintense signal alteration on the T2WI. There is no edema of the right ischiopubic synchondrosis or of the adjacent muscles and soft tissues.
Differential Diagnosis
The ischiopubic synchondrosis can be easily mistaken for other entities,
particularly osteomyelitis or tumor. It is often a diagnosis of exclusion as laboratory values are usually normal.
In the symptomatic child,
the radiographic findings can be more difficult to interpret,
and clinicians are more likely to assume these radiographic abnormalities are pathologic.
In acute hematogenous osteomyelitis limping,
fever and constitutional symptoms such as malaise and fatigue are more common.
Inflammation markers as erythrocyte sedimentation rate (ESR) and c-reactive protein (CRP) are also more commonly elevated in osteomyelitis.
The white blood cell (WBC) seems to be less helpful.
On MRI,
osteomyelitis patients have usually a much more diffuse enhancement of the IPS and they usually have surrounding myositis,
abscess,
and fluid collections.
In Van Neck-Odelberg there is normally only a focal area of marrow edema and resolution of symptoms occurs with simple observation.
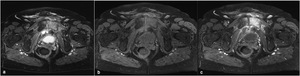
Fig. 6: Pelvic MRI of a 70-year old female with fever and groin pain, axial DP FS (a), axial FS T1 (b) and axial FS T1 post-contrast (c). The MR depicts marked signal changes of the left symphysis, with marked enhancement with contrast. There was also a collection involving the anterior contour of the symphysis and extending to the lower abdominal wall. The MRI and the clinical and laboratory context were suggestive of osteomyelitis.
Punctate calcifications on CT scans could represent chondral tumors,
such as enchondromas or chondrosarcomas,
but these are rare in children younger than 10 years old.
Ewing sarcoma has a high incidence before 10 years of age and the pelvis is one of the most common locations,
especially the ischiopubic region.
However,
the insidious development of complaints,
the bony nonspecific lytic lesions and considerable involvement of the soft tissues on MRI helps to differentiate this tumor from an enlarged IPS.


, and complete ossification 8 months later (b).")
 and soft tissue (b) window, showing an expansile lucent lesion in the left ischiopubic synchondrosis, with well-defined borders and no soft tissue component nor periosteal reaction.")
 and sagittal FS DPWI (b), showing bone marrow edema involving the left ischiopubic synchondrosis, with subperiosteal liquid. There is also marked swelling of the adjacent muscles.")
 and axial T2W images (b), showing a band-like hypointense area in the center of the left ischiopubic synchondrosis, consistent with fibrosis. One can also see swelling of the adjacent soft tissue as a hyperintense signal alteration on the T2WI. There is no edema of the right ischiopubic synchondrosis or of the adjacent muscles and soft tissues.")
, axial FS T1 (b) and axial FS T1 post-contrast (c). The MR depicts marked signal changes of the left symphysis, with marked enhancement with contrast. There was also a collection involving the anterior contour of the symphysis and extending to the lower abdominal wall. The MRI and the clinical and laboratory context were suggestive of osteomyelitis.")