ESSR 2019 / P-0100
Hydroxyapatite deposition and associated myositis: An imaging review
Congress:
ESSR 2019
Poster Number:
P-0100
Type:
Educational Poster
Keywords:
Musculoskeletal soft tissue, MR, Ultrasound, Conventional radiography, Education, Inflammation
Authors:
C. Azzopardi1, G. Kiernan2, J. Teh2; 1Oxford /UK, 2Oxford/UK
DOI:
10.26044/essr2019/P-0100
")
Fig. 1:
Plain X-ray of the right hip demonstrates amorphous dense calcification in the...
")
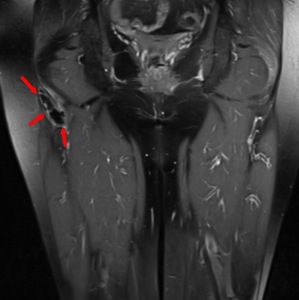
Fig. 2:
Coronal STIR image of the pelvis confirms the calcific depositis in the right...
 with a calcification in the peroneus longus origin (red arrow). Surrounding peri-calcific oedema is seen as a hypoechoic halo.")
Fig. 3:
B mode ultrasound of the proximal fibular head (star) with a calcification in...
 with marked reactive myositis")
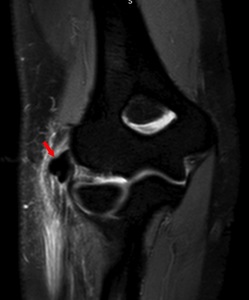
Fig. 4:
Sagittal PD fat saturated images of the knee demonstrate a calcific deposit in...
")
Fig. 5:
Plain radiograph of the right elbow shows a large dense calcification lateral...

Fig. 6:
Doppler image of the common extensor origin demonstrates avid vascularity...
 with striking myositis in the muscle belly of ERCB")
Fig. 7:
Coronal MR image demonstrates intra-tendinous calcification in the common...
 with straightening of the cervical spine")
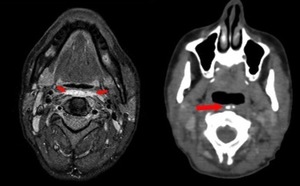
Fig. 8:
Subtle calcifications in the anterior soft tissues of the neck (red arrows)...
 demonstrates marked pre-vertebral oedema (red arrows) and corresponding axial non contrast CT (right) shows the co-existing pre-vertebral soft tissue calcifications (red arrows).")
Fig. 9:
Fat saturated T2 weighted axial MR image (left) demonstrates marked...

Fig. 10:
Sagittal STIR image of the cervical spine. Red arrows delineate the marked...