ESSR 2019 / P-0104
All about cystic lesions at the shoulder: Systematic review related to adjacent structures with MR imaging and illustration, with or without pathology.
Congress:
ESSR 2019
Poster Number:
P-0104
Type:
Educational Poster
Keywords:
Education, MR, Musculoskeletal joint, Anatomy, Cysts
Authors:
S. Lee1, E. K. Khil2, S.-Y. Park1, J.-A. Choi3, M. H. Lee4; 1Gyeonggi-do/KR, 2Hwaseong-si/KR, 3Seongnam, Gyeonggi-do/KR, 4Seoul/KR
DOI:
10.26044/essr2019/P-0104

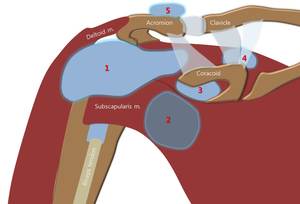
Fig. 1:
Bursa aorund the shoulder joint:
1. subacromial-subdeltoid bursa
2....

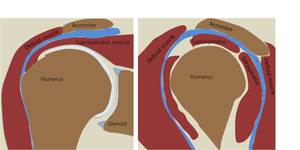
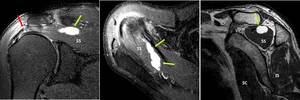
Fig. 2:
Subacromial-subdeltoid bursa:
The SA-SD bursa extends between the acromion and...
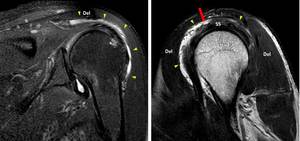
. Oblique coronal FS T2 and oblique sagittal T2 WI MR images show subdeltoid - subacromial bursa effusion (green arrow heads).
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
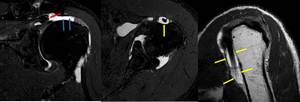
Fig. 3:
Subacromial-subdeltoid bursa:
73 year-old male with partial thickness...

Fig. 4:
Subscapular bursa = superior subscapular recess:
The subscapular recess lies...
.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 5:
Subscapular bursa without rotator cuff tear:
54 yeaer-old male without rotator...
.
Note combined SASD bursa (arrow head) and subscapular bursa (asterisk)
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
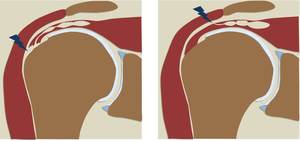
Fig. 6:
Subscapular bursa with rotator cuff tear:
55 year-old female with full...
. Joint effusion, subacromiao-subdeltoid bursa effusion (blue asterisk), and subscapular bursa effusion (red asterisk) are presented.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 7:
Subscapular bursa with rotator cuff tear:
65 year-old male with full-thickness...
. Large amount of effusion is presented in shoulder joint and subscapular bursa (asterisk). Isosignal intensity is filled in joint space, suggestive of synovial proliferation (yellow arrow).
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 8:
Subscapular bursa with rotator cuff tear and synovitis:
73 year-old female...

Fig. 9:
Subscapular bursa associated inflammatory arthritis:
32 year-old male with...
, suggestive of R/O internal hemorrhage.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
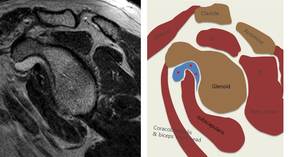
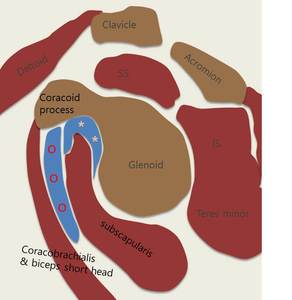
Fig. 10:
Subscapular bursa with fluid-fluid level:
70 year-old female with massive full...
 lies between the subscapularis tendon inferiorly, and the coracoid process and the combined tendon of the short head of the biceps and the coracobrachialis muscle superiorly.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
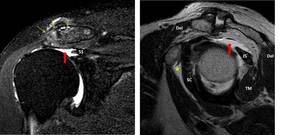
Fig. 11:
Subcoracoid bursa:
The subcoracoid bursa (circles) lies between the...
 and subcoracoid bursa effusion (asterisk) on cornal and sagittal T2-WI.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 12:
Subcoracoid bursa:
62 year-old male with right shoulder pain.
There is no...
. Subscapular bursa effusion (blue asterisk) is also noted.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 13:
Subcoracoid bursa with rotator cuff tear:
65 year-old female with full...
. Oblique sagittal T2-WI MR image shows accompanying subcoracoid bursa effusion (blue asterisk). Note septa (yellow arrow) in subcoracoid bursa (blue asteirsk). There is communication (red arrow) between subacromial-subdeltoid bursa (green arrow head) and subcoracoid bursa (blue astiersk).
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 14:
Subcoracoid bursa with rorator cuff tear and communication with SA-SD...
, about 2cm length) and partial thickness tear of supraspinatus tendon (yellow thick arrow). Subacromial-subdeltoid bursa (arrow head) and subcoracoid bursa (blue asterisk) effusion is demonstrated.
Note multiseptated (red thin arrow) subcoracoid bursa.
Associated moderate atrophy of the rotator cuff muscles is shown.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 15:
Subcoracoid bursa:
65 year-old female with full-thickness tear of...
 and infraspinatus tendon, associated severe atrophy in supra- & infra- spinatus muscle. There is underlying severe osteoarthritis with spur formation and capsular distension in acromioclavicular joint (green arrow). Note the subcoracoid bursa effusion (asterisk)
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 16:
Subcoracoid bursa:
73 year-old female with massive tear of supraspinatus...

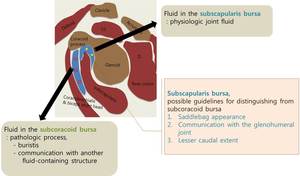
Fig. 17:
Subscapular bursa VS. subcoracoid bursa:
The distinction between the two...

Fig. 18:
Intramuscular cyst:
Possible explanation for the association of intramuscular...
. There is multiloculating intramuscular cysts (green arrow) in supraspinatus muscle. Mild atrophy of supraspinatus and infraspinatus muscles are also noted.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 19:
Intramuscular cyst – SST:
62 year-old male with right shoulder pain. Oblique...
, associated mild atrophy of supra- and infra- spinatus muscle and teres minor muscle.
Threre is multiloculated intramuscular cyst (green arrow) in supraspinatus muscls.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 20:
Intramuscular cyst – SST:
53 year-old male with full-thickness tear of...
.
However, Note intramuscular cyst (green arrow) in the sibscapularis muscle without definite evidence of subscapularis tendon tear
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 21:
Intramuscular cyst – SCT:
65 year-old male with Partial tear of...
 is noted in subscapularis muscle with/without subscapularis tendon tear.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 22:
Intramuscular cyst – SCT:
52 year-old male with underlying HCC. There is...
 and small intramuscular cyst (yellow arrow) at myotendinous junction of infraspinatus.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 23:
Intramuscular cyst – IST:
73year-old male with left shoulder pain. There is...

Fig. 24:
Fluid collection of the biceps tendon sheath:
The biceps tendon sheath is an...
.
See the retracted supraspinatus tendon (red arrow). There is moderated amount of glenohumeral joint effusion. Also noted fluid collection along the biceps tendon sheath (yellow arrow).
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 25:
Fluid collection of the biceps tendon sheath associated with rotator cuff...

Fig. 26:
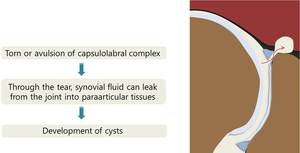
Paralabral cyst:
That the principal cause of a paralabral cyst is an adjacent...
 in anterosuperior aspect of glenoid
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
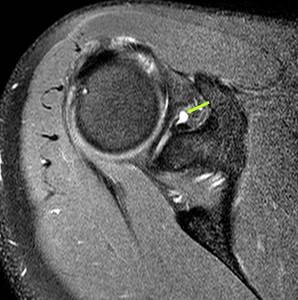
Fig. 27:
Paralabral cyst:
32 year-old male. Axial FS T2 MR image demonstrates
SLAP...
. Possibility of associated labral tear was reported. On arthroscope, anterior labral degeneration was confirmed.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 28:
Paralabral cyst:
59 year-old male. Axila and oblique coronal FS T2 MR images...
.
Also noted associated paralabral cyst (green arrow).
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 29:
Paralabral cyst:
41 year-old male with crepitus, right shoulder.
Axial and...
 lesion (red arrow).
Note the contrast leakage which is forming a paralabral cyst (green arrow) at superoposterior portion of superior glenoid
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 30:
Paralabral cyst:
57 year-old male taken right shoulder MR arthrography. Axial...
 along the posterior labrum without labral tear.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 31:
Paralabral cyst:
55 year-old female with right shoulder pain.
Note...
 in posterior portion of glenoid.
There is no evidence of labral tear on conventional shoulder MR.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 32:
Paralabral cyst:
48 year-old male with small labral cyst (green arrow) in...
 in posterior aspect of the labrum with linear high signal intensity (red arrow) in 9 to 10 o’clock direction of the labrum. Rotator cuff is intact.
Tiny paralabral cyst (green arrow) with labral tear (red arrow) is reported.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 33:
Paralabral cyst:
20 year-old male with right shoulder pain.
There is a tiny...

Fig. 34:
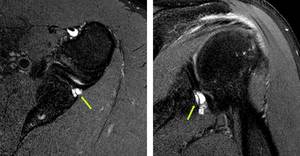
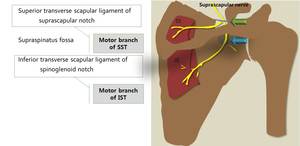
Ganglion cysts with entrapment neuropathy of suprascapular...

Fig. 35:
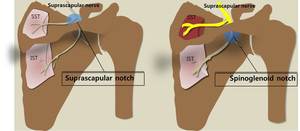
Ganglion cysts with entrapment neuropathy of suprascapular nerve:
Paralabral...
 at the anteroinferior aspect of the supraspinatus muscle within the coracoacromial arch of the right shoulder, extension to the suprascapular notch and spinoglenoid fossa.
Mild atrophy of supraspinatus and infraspinatus muscle was suspected.
Ganglion cyst causing suprascapular nerve entrapment was diagnosed on MR.
Ganglion cyst was confirmed through excisional biopsy.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
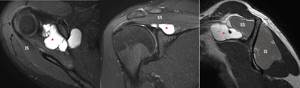
Fig. 36:
Ganglion cyst at suprascapular notch:
27 year-old male with right shoulder...
 is presented at left spinoglenoid notch.
Note increased signal intensity of infraspinatus muscle on T2WI, suggestive of suprascapular nerve entrapment.
Ganglion cyst was confirmed through excisional biopsy.
References: Radiology, Ulsan University Seoul Asan Hospital - Seoul/KR")
Fig. 37:
Ganglion cyst at spinoglenoid notch:
34 year-old male with left shoulder pain....