Procedure
A selection of representative cases of adolescent and young adults (aged between 15 and 40 years old) with pathologically proven primary malignant bone tumor was used to illustrate imaging findings and to highlight the role of plain radiography,
CT and MRI in bone tumor diagnosis,
staging and follow-up.
Fundamental criteria for categorizing an osseous Lesion on conventional radiography
1.
Pattern of bone destruction and lesion margin
- Analysis of the transition zone (width of the margin between normal bone and abnormal bone)
- Identification of the presence / absence of sclerosis at the tumor margin
According to the analysis of the transition zone and the presence/absence of sclerosis,
a lytic osseous lesion can be categorized into five types (see Fig. 1)
Endosteal scalloping: a medullary tumor can cause a well defined destruction of cortical bone in its inner margin
- Less agressive lesions --> bone expansion as the periosteum can maintain an intact layor of overlying bone
- Highly aggressive lesions --> bone destruction may progress to cortical breakthrough
2.
Lesion density
- Lesion purely lytic (radiolucent)
- Lesion purely blastic (radiodense)
- Lesion mixed (lytic and blastic)
3.
Tumor matrix
- Osteoid matrix: mineralization is dense,
homogeneous/amorphous,
"cloud-like" (bone island; osteoid osteoma; osteoblastoma; Osteosarcoma)
- Chondroid matrix: calcifications in the form of "arcs and rings", “punctate” and “popcorn" (enchondroma; cap of osteochondroma; chondroblastoma; chondromyxoid fibroma; chondrosarcoma)
-
Intermediate matrix: Diffuse uniform mineralization "ground glass" (fibrous dysplasia,
osteoblastoma)
-
Cellular matrix: no calcifications,
radiolucent lesions (fibrous tumors and round cell tumors)
4.
Location of lesion
There are three aspects which are important regarding localisation of lesion in determining its probable diagnosis,
namely:
- Specific bone where the lesion is found (tibia,
femur,
etc.) or category of bones (such as flat vs.
long; apendicular vs.
axial skeleton)
- Location along the length of a bone (metaphyseal; epiphysis; diaphyseal)
- Location in the transverse plane of a bone (central; eccentric; cortical; parosteal)
5.
Periosteal reaction
Periosteal reaction can be described as uninterrupted ("solid") versus interrupted
Uninterrupted periosteal reaction ("solid") corresponds to uniform cortical thickening (see Fig. 6)
- Reflects a slow-growing lesion or benignity
Interrupted periosteal reaction is seen with rapidly progressive lesions such as maligant tumors or osteomyelitis and include the following types (see Fig. 6):
6.
Age of patient
Knowledge of patient’s age is fundamental to the correct interpretation of imaging findings.
In fact,
there is a propensity of certain tumors or tumor-like lesions to affect specific age groups of patients.
CT
Although MRI is preferred for local staging both in osseous and soft tissue tumors,
it can still be useful for:
- Evaluation of tumor margins,
matrix mineralization,
and cortical breakthrough
- Detecting mineralization and bone involvement
- Visualizing soft tissue masses and defining compartmental involvement
- Assessment of lipomas,
calcified lesions and myositis ossificans
- Useful to guide percutaneous bone biopsy
MRI
When a lesion has radiographic features that are indeterminate or aggressive and considered to be potentially malignant,
MRI is useful for further characterization as well as staging.
MRI allows to assess some tissue characteristics such as fat,
hemorrhage,
fibrous tissue and fluid–fluid levels and the administration of gadolinium contrast is useful to evaluate tumor vascularity and also to distinguish cystic,
myxoid or necrotic from solid component.
The permeative nature of a lesion is better evaluated on radiograph and CT than MRI,
as well as the type of periosteal reaction.
Staging of Bone Tumors
Two staging systems are currently used:
- TNM staging system designed by the American Joint Committee on Cancer (AJCC)
A major characteristic of TNM classification in bone sarcomas is that histopathologic grade (G) is included as a factor in staging. In the eighth edition,
the histologic grading system have changed to a three-grade classification and the bone sarcomas are now separately described according to the primary tumor site: a) appendicular skeleton,
trunk,
skull and facial bones; b) spine; c) pelvis.
This staging system is applied for all primary bone sarcomas,
except primary malignant lymphoma and multiple myeloma.
- Musculoskeletal Tumor Society (MSTS) surgical staging or Enneking surgical staging system for malignant mesenchymal tumors
Takes into account the surgical grade (G,
G1,
G2),
local extent (T,
T1,
T2),
and presence or absence of metastasis (M0,
M1).
Local extent refers to its containment in anatomic boundaries of a compartment which have inherent barriers to tumor spread,
including fascial planes and bone structures.
The approach for surgical procedure is mainly determined by local tumor extent.
Restaging of Bone Tumors
Conventional osteosarcomas,
as well as several other highgrade sarcomas,
are treated with preoperative chemotherapy.
The restaging includes chest CT to evaluate for lung metastases and also MRI in all 3 planes with contrast administration.
Comparison with pretherapy imaging must include evaluation of any change in size of the lesion, degree of necrosis,
and assessment of any tissues that now appear to be free or involved of tumor.
A good response is not necessarily associated with significant tumor shrinkage on imaging studies.
Indeed, osteosarcoma may paradoxically appear to enlarge on posttherapy imaging due to maturation of previously deposited osteoid matrix.
OSTEOSARCOMAS
Several types of osteosarcoma are recognised because of their different imaging features,
prognosis and treatment.
1.
CONVENTIONAL (HIGH-GRADE INTRAMEDULLARY) OSTEOSARCOMA
Definition: malignant osteoid-producing tumor originating in intramedullary space
1.1) Clinical features:
- Most common malignant bone tumor in children/adolescents (75% of all osteosarcomas)
- Most arise in children and young adults between 10 - 25 years of age (male > female)
- 5-10% have pulmonary metastases at presentation
1.2) Imaging features
1.2.1) Location Fig. 2
- The majority (90%) are metaphyseal; can be diaphyseal
- 75-88% extension to epiphysis in children (physis is not effective barrier)
- Occurs most commonly at the sites of most rapid growth: distal femur > proximal tibia > proximal humerus
1.2.2) Radiographic findings
- Poorly defined intramedullary lytic and aggressive lesion (wide zone of transition,
permeative pattern),
eccentric with varying degrees of osteolysis and osteosclerosis (most frequent)
- Osteoid matrix
- Cortical destruction associated with an interrupted periosteal reaction (such as Codman’s triangle,
“hair-on-end”,
“sunburst” and “onion skin”)
- Large soft tissue masses are seen in tumors with cortical disruption
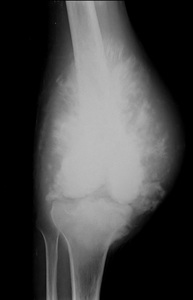
Fig. 7: High-grade intramedullary osteosarcoma of the distal femur in a 22 years old male patient.
Anteroposterior radiograph of the knee shows extensive mineralized osteoid throughout the ill defined osteobbastic lesion, aggressive periosteal reaction (sunburst type) and soft-tissue extension.

Fig. 8: High-grade intramedullary osteosarcoma of the distal femur in 19 years old male patient.
1.2.3) CT Findings
- May better define the osteoid matrix
- Required for staging of lung metastases (may be ossified)
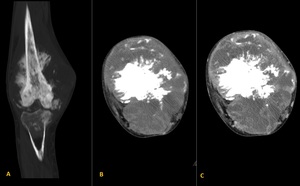
Fig. 9: High-grade intramedullary osteosarcoma of the distal femur in a 22 years old male patient (same patient of figure 7). Coronal and axial non-enhanced CT images (A and B) reveals an extensive and ill defined osteoblastic lesion with an aggressive periosteal reaction (sunburst type) and soft-tissue extension which shows contrast enhancement (image C).
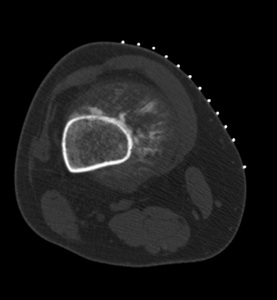
Fig. 10: Axial non-contrast enhanced CT of a patient with an high-grade intramedullary osteosarcoma of the distal femur (same patient of figure 8).
1.2.4) MRI findings
- Osteoid matrix: low signal on all sequences
- Non osteoid portions near isointense to muscle on T1
- Fluid-sensitive sequences (generally fat saturated): heterogeneous increase signal in soft tissue and osseous mass; peritumoral edema (may exaggerate size of mass)
- Intense enhancement of marrow and soft tissue mass (differentiates viable regions from necrosis)
- Detect “skip” lesions (metastatic lesions to the same bone) occuring in 1% to 10% of cases
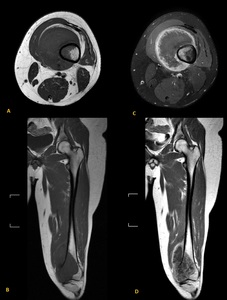
Fig. 11: Axial and coronal T1-weighted images obtained before (A and C) and after intravenous administration of contrast (B and D) material reveals the extent of enhancing marrow and soft-tissue involvement (same patient of figure 8 and 10).
Differential diagnosis:
- Ewing’s sarcoma: the reactive bone formation is restricted to the involved bone and does not extend into the soft tissue mass in a Ewing’s sarcoma
2.
TELANGIECTATIC OSTEOSARCOMA
Definition: Malignant bone-forming tumor containing or largely consisting of large blood-filled spaces
2.1) Clinical features:
- Rare (4-12% of osteosarcomas) ocurring in the same group age and location as conventional osteosarcoma
- 5-year survival rate and treatment similar to conventional osteosarcoma
2.2) Imaging features
2.2.1) Location
- 90% long bone metaphysis: distal femur > proximal tibia > proximal humerus > proximal femur
- Other locations are rare
2.2.2) Radiographic findings

Fig. 12: Telangiectatic osteosarcoma in a 32 years old male patient with Osteogenesis imperfecta type III. The knee radiograph reveals a lytic with aneurysmal expansion of the cortex expansile in the metaphysis and epiphysis of the tibia.
2.2.3) CT Findings
- Heterogeneous low attenuation in center of lesion
- Small calcific foci in periphery: better seen on CT than on radiograph
- Fluid-fluid levels present but only visible in 48% of cases
- Cortical destruction and soft tissue mass
- Enhancement of tumor at periphery and in septa
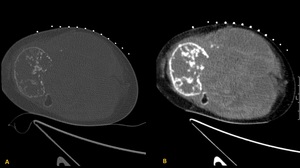
Fig. 13: Axial non–enhanced CT images (A and B) shows a markedly expansile lytic lesion with cortical destruction in the metaphysis and epiphysis of the tibia with multiple septa within the soft tissue mass
2.2.4) MRI findings
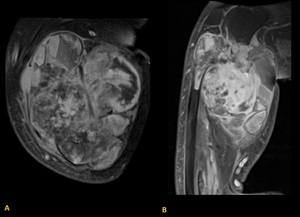
Fig. 14: Axial and Sagital T1-weighted images revealing inhomogeneous signal similar to or slightly higher than muscle intensity with multiple fluid-fluid levels.
Differential diagnosis:
The metastatic potential,
work-up,
prognosis,
and therapy are identical to those for conventional osteosarcoma.
PAROSTEAL OSTEOSARCOMA
Definition: Low-grade osteosarcoma arising on surface of bone
2.1) Clinical features:
- 2nd most common type of osteosarcoma (>80% of cases)
- Occur between the ages of 20 - 50 years
- One of the few sarcomas that is not more common in males (male-to-female ratio 2:3)
-
Usually low grade and better differentiated than conventional and telangiectatic osteosarcoma --> better prognosis
-
Metastases to the lung occur later and with less frequency than with conventional osteosarcoma
2.2) Imaging features
2.2.1) Location
-
More frequent at the posterior distal femoral metaphysis
-
Although the site of origin is the bone surface,
the tumor is located nearly entirely in the soft tissues with lobulated margins
2.2.2) Radiographic findings
-
Lesion arises from cortical surface: i) may develop as cortical thickening,
partially circumferential,
which contains mixture of disorganized dense bone formation and lytic regions; ii) appearance of cleft (seen on radiograph in 30% of cases)
- Tumor matrix is usually densely sclerotic centrally while peripherally is less mature or even nonossified - this zoning pattern is the reverse of myositis ossificans

Fig. 15: Low grade parosteal osteosarcoma of the foot (2nd metatarsal bone) in a 20 years old male patient. The lesion appears as partially circumferential but ill defined containing a mixture of disorganized dense bone formation and lytic regions
2.2.3) CT Findings
- Mimics those of radiograph but better depicted - cleft better seen in 65% of cases;
- Easier to evaluate maturity and zoning of osseous matrix

Fig. 16: Low grade parosteal osteosarcoma of the foot (2nd metatarsal bone) in a 20 years old male patient. Coronal, sagital and axial CT images reveals an ossified exophytic tumor on the surface of the 2nd metatarsal bone with a lucent line seen between the tumor and underlying bone (corresponding to the periosteum).
2.2.4) MRI findings
- T1: low signal intensity osseous mass; heterogeneous signal isointense to skeletal muscle in soft tissue mass
- Marrow involvement in approximately 50% of cases
- Enhancement of soft tissue and involved marrow
- regions of lesion that have more aggressive or different appearance (such as fluid levels) may represent higher grade
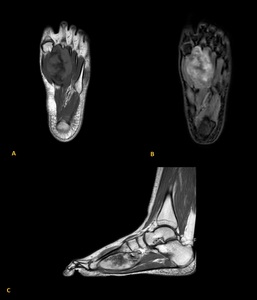
Fig. 17: Low grade parosteal osteosarcoma of the foot (2nd metatarsal bone) in a 20 years old male patient. T1-weigted images before (A) and after gadolinium injection reveals (B and C) reveals a low signal intensity osseous mass with heterogeneous signal and enhancement of soft tissue
Differential diagnosis:
PERIOSTEAL OSTEOSARCOMA
Definition: Intermediate-grade surface osteosarcoma, commonly
chondroblastic
2.1) Clinical features:
-
Occur in the second or third decade of life
-
Prognosis is better than that of conventional osteosarcomas,
but not as good as that of parosteal osteosarcomas
2.2) Imaging features
2.2.1) Location
2.2.2) Radiographic findings
-
The soft tissue mass extends from the surface of the lesion,
usually with calcified spicules of bone emanating in a sunburst pattern
- May have little bone formation visible on radiograph
- Zoning pattern of maturation typical of surface osteosarcomas
- Scalloping of the underlying cortex and cortical thickening may occur
-
Periosteal reaction is often in the form of Codman’s triangle

Fig. 18: Periosteal osteosarcoma in the diaphysis of the femur in a 18 years old male patient. The radiograph reveals an oblong dense lesion arising from the diaphyseal surface of the femur with irregular thickening of the adjacent cortex. A Codman’s triangle and radiating or cloud-like
osseous proliferation is seen.
2.2.3) CT Findings
- Similar to the findings on radiography but more clearly delineated
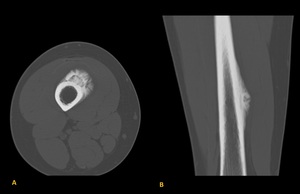
Fig. 19: Periosteal osteosarcoma in the diaphysis of the femur in a 18 years old male patient. CT reveal similar findings to radiography but are more clearly delineated.
2.2.4) MRI findings
- T1: low signal intensity of cortex and osteoid; soft tissue mass tends to be isointense to skeletal muscle
- Fluid-sensitive sequences: low signal osteoid matrix extending as rays perpendicular to cortex; heterogeneous high signal intensity soft tissue mass,
extending from periphery of osteoid matrix;
- High signal within fat-saturated marrow,
contiguous with tumor indicates marrow extension (uncommon)
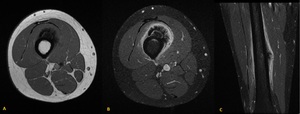
Fig. 20: Periosteal osteosarcoma in the diaphysis of the femur in a 18 years old male patient. T1-weighted images demonstrastes low signal intensity of cortex and osteoid and soft tissue mass tends to be isointense to skeletal muscle. On fluid-sensitive sequences the lesion reveals low signal osteoid matrix extending as rays perpendicular to cortex and heterogeneous high signal intensity soft tissue mass extending from periphery of osteoid matrix.
Differential diagnosis:
EWING’S SARCOMA
Definition: round-cell sarcoma of bone that occurs predominantly in the long bones of skeletally immature patients
2.1) Clinical features:
-
Most common primary malignant bone tumor found in children
in the first decade of life
-
Rare in black patients
-
15-30% have metastasis at the time of diagnosis (frequency lung metastasis = bone metastasis)
2.2) Imaging features
2.2.1) Location Fig. 3
2.2.2) Radiographic findings
2.2.3) CT Findings
- Required for staging for lung metastases
- Mimic radiographic findings: Focal cortical destruction seen well; subtle linear cortical channels extending to soft tissue mass common (66%)
- Only evidence of cortical destruction in 30% of cases
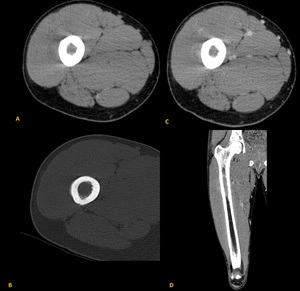
Fig. 21: Ewing's sarcoma in a 25 years old male patient.
2.2.4) MRI findings
- Non specific appearance: low to intermediate signal intensity on T1 and T2-weighted images
- Soft tissue component of the mass is large and may contain central necrosis
- High signal periosteal reaction
- Marrow and soft tissue edema
- Linear canals connecting marrow to soft tissue mass (highly suggestive of round cell tumor)
- Heterogeneous and avid enhancement on postcontrast imaging
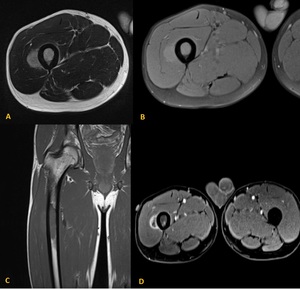
Fig. 22: MRI images of a Ewing's sarcoma localized on the metadiaphysis of the femur in a 25 years old male patient. The tumor demonstrates low to intermediate signal intensity on T1 and T2-weighted images with high signal periosteal reaction, marrow and soft tissue edema, showing heterogeneous and avid enhancement on postcontrast imaging.
Differential diagnosis:
- Osteomyelitis: MRI with contrast usually sllows to distinguis them due to thickwalled soft tissue abscesses and intramedullary abscess in osteomyelitis
- Osteosarcoma: most have some degree of osteoid matrix
- Langerhans Cell Histiocytosis: may reveal faster osseous destruction; soft tissue mass is usually smaller
- Lymphoma: can be have a very similar appearance
PRIMARY LYMPHOMA OF BONE
Definition: Neoplasm composed of malignant lymphoid cells in the absence of involvement of distant lymph nodes or viscera for 6 months following diagnosis
- Single skeletal site ± regional lymph node involvement
- Multiple bone involvement without visceral or lymph node involvement (primary multifocal osseous lymphoma)
2.1) Clinical features:
-
Incidence increases with age throughout life
-
Wide range but most common from 30 to 60 years
- 11-31% are multifocal at initial presentation (more frequent in children than adults)
-
Lung metastases are uncommon,
but when present may increase in size and number quickly
2.2) Imaging features
2.2.1) Location Fig. 5
- Regions of persistent red marrow
- Lesion tends to arise in appendicular central diaphyseal or metadiaphyseal sites, more commonly in the femur,
tibia and humerus
2.2.2) Radiographic findings
2.2.3) CT Findings
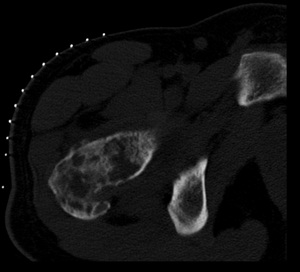
Fig. 23: Non-Hodgkin lymphoma (diffuse large B-cell lymphoma) of the proximal femur in a 22 years old male patient.
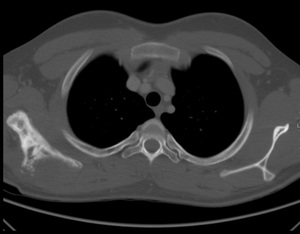
Fig. 24: Non-Hodgkin lymphoma (diffuse large B-cell lymphoma) of the scapula in a
17 year old male patient.
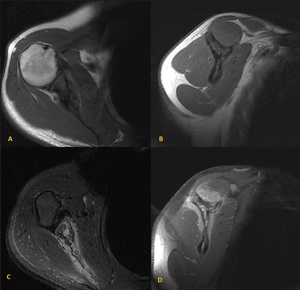
Fig. 25: Non-Hodgkin lymphoma (diffuse large B-cell lymphoma) of the scapula in a
17 year old male patient.
Axial and sagital T1-weighted-images before (A and B) anf after gadolinium administration (C and D). Hypointense lesion on T1 of the scapula with soft tissue component demonstrating contrast enhancement.
2.2.4) MRI findings
2.2.5) Differential diagnosis:
Chondrosarcoma
Definition: Malignant hyaline cartilage tumor
Chondrosarcomas are categorized according to:
- Location within the bone (central,
peripheral or juxtacortical)
- Arising as a new lesion (primary chondrosarcoma) or on a preexisting lesion such as an osteochondroma or enchondroma (secondary chondrosarcoma)
- Degree of cellular differentiation (low grade,
medium grade,
or high grade)
We will refer to conventional chondrosarcomas which includes central and peripheral types.
In general,
central chondrosarcomas tend to be primary,
and peripheral chondrosarcomas tend to arise from pre-existing lesions
2.1) Clinical features:
- Chondrosarcoma occurs most frequently in the fourth to sixth decades of life but age should not be used to exclude the diagnosis in a teenager or young adult
- The majority of central chondrosarcomas are low grade
2.2) Imaging features
2.2.1) Location Fig. 4
-
Iliac wing > proximal femur > proximal humerus > distal
femur
-
Metaphyseal or metadiaphyseal
-
Epiphyseal lesion is uncommon but should raise a red
flag: a chondroid lesion that is not chondroblastoma at this site should raise suspicion
2.2.2) Radiographic findings
Central chondrosarcoma
- Central lytic lesion arising in metaphysis or diaphysis
- Chondroid matrix usually present
- If low-grade lesion there is limited appearance of aggressiveness on radiograph
- Endosteal scalloping that removes more than two thirds of the cortical thickness favors a chondrosarcoma over an enchondroma
- Usually no periosteal reaction
- Little or no cortical breakthrough/soft tissue mass
Peripheral chondrosarcoma
- Analysis of previous routine radiography helps to distinguish between a benign osteochondroma and one that has undergone malignant transformation
- Suspicious features for malignancy: i) bulky cartilaginous cap;ii) irregular or indistinct surface of the calcified tissue beneath the cartilaginous cap; iii) scattered calcifications in the cartilaginous part of the tumor; iv) focal areas of radiolucency in the interior of the osteochondroma; v) soft tissue mass and destruction/erosion of the adjacent bone
2.2.3) CT Findings
• Mimics radiographic findings but changes are usually beter seen, being useful to analyze intraosseous and soft tissue extent and also to identify matrix and erosive changes
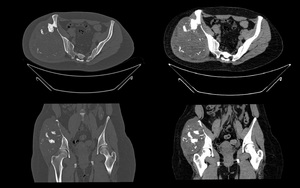
Fig. 26: Chondrosarcoma of the iliac wing in a 29 years old female patient. Axial and coronal CT images reveals a large exophytic mass with soft tissue component and chondroid calcification seen at right side of pelvis arising from right iliac bone with aggressive features such as lytic pattern, deep endosteal scalloping and soft-tissue extension.
2.2.4) MRI findings
- Allows to identify the full extent of the tumor and to better define endosteal scalloping (central chondrosarcomas)
- T1-weighted images: hypointense to muscle
- T2-weighted images: multilobulated high signal intensity lesion
- Earlier enhancement in chondrosarcoma on fast contrast-enhanced gradient-echo MR may help differentiate enchondroma from low-grade chondrosarcoma but significant overlap exists
- Peripheral chondrosarcoma: cartilage cap seen as high signal intensity on fluid-sensitive images with thickness > 1 cm; higher-grade lesions may show destruction of the stalk as well as soft tissue mass beyond the cartilaginous cap
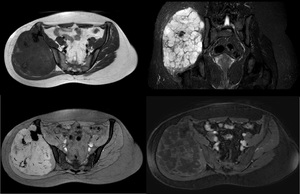
Fig. 27: Chondrosarcoma of the iliac wing in a 29 years old female patient. The lesion is hypointense to muscle on T1-weigthed images (A) and hyperintense on T2 FFE (B) and STIR (C) with multilobulated appearance revealing contrast enhancement (D)
Differential diagnosis:






