ESTI ESCR 2018 / P-0015
Evaluation of the anatomical distribution of pulmonary emboli on CT pulmonary angiography
Congress:
ESTI ESCR 2018
Poster Number:
P-0015
Type:
Scientific Poster
Keywords:
Pathology, Embolism / Thrombosis, Acute, Observer performance, Education, CT-Angiography, CT, Vascular, Pulmonary vessels, Cardiovascular system
Authors:
S.-M. O'Hanlon, T. Wooding, A. Mittal, Y. D. Weerakkody; Perth/AU
DOI:
DOI-Link:
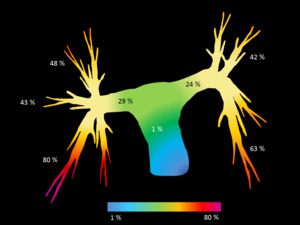
 to purple (areas of highest embolic burden). References: Yuranga Weerakkody")
Fig. 2:
Diagramatic representation of the percentage prevalence of emboli within the...

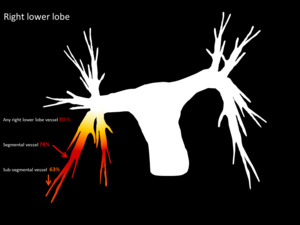
Fig. 3:
Segmental and subsegmantal distribution of embolic burden in right lower lobe...

Fig. 4:
Segmental and subsegmantal distribution of embolic burden in right upper lobe...

Fig. 5:
Segmental and subsegmantal distribution of embolic burden in right middle lobe...

Fig. 6:
Segmental and subsegmantal distribution of embolic burden in left upper lobe...

Fig. 7:
Segmental and subsegmantal distribution of embolic burden in left lower lobe...

Fig. 8:
Prevalence of emboli classified by vessel location, expressed as a percentage...

Fig. 9:
Prevalence of emboli classified by horizontal and vertical location, expressed...

Table 1:
Associated CT features

Table 2:
Largest vessel involved: central versus peripheral

Table 3:
Male versus female clot distribution

Table 4:
Clot distribution according to presence or absence of COPD changes

Table 5:
Clot burden distribution according to presence or absence of a history of...