ECR 2007 / C-336
Congenital mullerian anomalies: Three-dimensional ultrasound findings
Congress:
ECR 2007
Poster Number:
C-336
Type:
Scientific Exhibit
Keywords:
Authors:
M. E. Belloch Ramos, F. Raga Baixauli, P. Naranjo Romaguera, F. Bonilla Bartret, F. Bonilla Musoles, J. Palmero da Cruz; Valencia/ES
DOI:
DOI-Link:

Fig. 1:
FIGURE 2. DISTRIBUTION OF MÜLERIAN DUCT ANOMALIES.
, transverse (b), coronal oblique 2D (c), and coronal oblique reconstructed 3D (d) endovaginal US image demonstrate fundal indentation and normal external uterine contour.")
Fig. 2:
Figure 3. ARCUATE UTERUS. Sagittal (a), transverse (b), coronal oblique 2D (c),...
, transverse (b), coronal oblique (c) 2D; and 3D reconstructed coronal oblique (d) endovaginal US images of a partial uterine septum demonstrate mild indentation of the uterine fundus with normal external contour.")
Fig. 3:
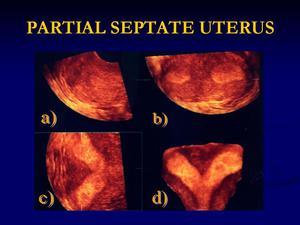
FIGURE 4a. PARTIAL SEPTATE UTERUS. Sagittal (a), transverse (b), coronal...
, transverse (b), coronal oblique (c) 2D; and 3D reconstructed coronal oblique (d) endovaginal US images of a partial uterine septum show convex external uterine contour with vertical septum extending to external uterine os.")
Fig. 4:
FIGURE 4b. COMPLETE SEPTATE UTERUS. Sagittal (a), transverse (b), coronal...
, transverse (b), coronal oblique (c) 2D; and 3D reconstructed coronal oblique (d) endovaginal US images demonstrate external fundal cleft with wide divergence of endometrial cavities.")
Fig. 5:
FIGURE 5. BICORNUATE UTERUS. Sagittal (a), transverse (b), coronal oblique (c)...
, transverse (b), coronal oblique (c) 2D; and 3D reconstructed coronal oblique (d) endovaginal US images show complete duplication of uterine horns and cervices.")
Fig. 6:
FIGURE 6. DIDELPHYS UTERUS. Sagittal (a), transverse (b), coronal oblique (c)...
, transverse (b), coronal oblique (c)2D; and 3D reconstructed coronal oblique (d) endovaginal US images demonstrate uterus with abnormal lenticular shape of endometrial cavity.")
Fig. 7:
FIGURE 7a. UNICORNUATE UTERUS. Sagittal (a), transverse (b), coronal oblique...
, transverse (b), coronal oblique (c) 2D; and 3D reconstructed coronal oblique (d) endovaginal US images show unicornuate uterus with rudimentary horn. Cavitary rudimentary horn is not communicated with the endometrium of the contralateral horn.")
Fig. 8:
FIGURE 7b. UNICORNUATE UTERUS WITH RUDIMENTARY HORN. Sagittal (a), transverse...
 extending to the external os. The fundus has a convex external contour (blue arrow).")
Fig. 9:
FIGURE 8. MR COMPLETE SEPTATE UTERUS. Coronal- oblique T2 weighted FSE image...

Fig. 10:
FIGURE 9. HYSTEROSALPINGOGRAPHY OF AN ARCUATE UTERUS. This study demonstrates a...
 shows two horns with wide divergence. Hysteroscopic image demonstrates two endometrial cavities within each horn.")
Fig. 11:
FIGURE 10. LAPAROSCOPY AND HYSTEROSCOPY OF A BICORNUATE UTERUS. Laparoscopy...