Type:
Educational Exhibit
Authors:
V. Pineda, X. Merino, J. Rodriguez, H. Cuellar, S. Gispert, R. Dominguez; Barcelona/ES
DOI:
10.1594/ecr2009/C-168
Imaging findings OR Procedure details
Why cardiac MRI?
- Cardiac MRI is able to distinguish between different causes of acute pain in patients with unobstructed coronary arteries.
- Because of its ability to noninvasively assess morpholgy,function, and tissue characteristics in a "one-stop shop" modality, cardiac MRI has become the method of choice in these patients.
Fig.
Which sequences?
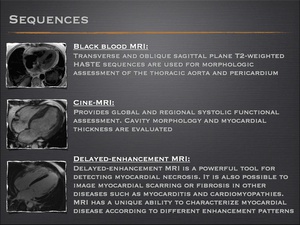
Fig.
What should be suspected?
The cardiac causes considered in the differential diagnosis of these patients include ischemic disease, myocarditis/perimyocarditis, cardiomyopathies and acute aortic syndrome.
Fig.
Ischemic disease
Acute myocardial infarction (AMI)
- Approximately 6% of patients with an AMI have angiographically normal coronary arteries.
- Myocardial infarction with normal coronary arteries primarily affects younger persons and is related to numerous conditions, but the exact pathophysiology remains unknown.
- DCE MRI is an accurate, sensitive technique for detecting myocardial infarction.
- Involvement starts near the endocardial surface of the left ventricle and progresses towards a more transmural infarction.
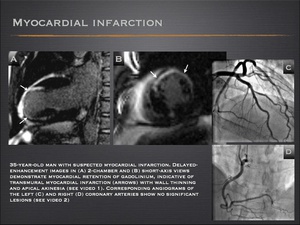
Fig.: Myocardial infarction
Coronary artery spasm
- Coronary artery spasm is usually suspected in patients with chest pain and angiographically normal coronary arteries.
- Cardiac MRI is a powerful tool for detecting myocardial infarctions, but cannot diagnose coronary artery spasm. Usually, findings are normal or mild regional wall motion dysfunction is seen.
- Cardiac MRI can exclude AMI, but the definitive diagnosis of vasospasm is made on angiographic evidence of coronary vasoconstriction that reverses with administration of intravenous or intra-arterial nitroglycerin. To confirm the diagnosis, intracoronary acetylcholine can be infused to induce arterial spasms.
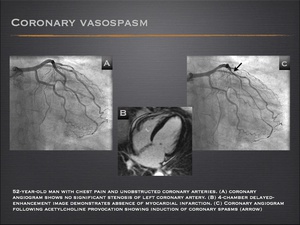
Fig.: Coronary artery spasm
Cardiac syndrome X
- Cardiac syndrome X defines patients with typical chest pain, transient ischemic ST segment changes on exertion, normal coronary angiograms, and no evidence of coronary artery spasm.
- Although the origin is unknown, one possibility is an ischemic origin related to endothelial dysfunction at the microvascular level. Patients with syndrome X may demonstrate reduced myocardial perfusion reserve at contrast-enhanced cardiac MRI with absence of myocardial scarring or infarction.
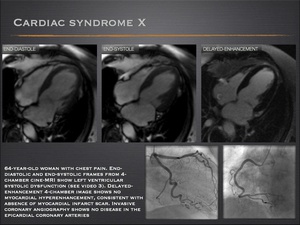
Fig.: Cardiac syndrome X
Myocarditis / perimyocarditis
- The clinical presentation of myocarditis can include chest pain, ischemic-like electrocardiographic abnormalities, elevated serum troponin levels, or segmental ventricular dysfunction. Therefore, the differential diagnosis with acute coronary syndrome remains difficult.
- Myocarditis frequently causes sufficient myocardial injury and scarring to result in delayed gadolinium enhancement on MRI.
Myocarditis shows a characteristic pattern of contrast enhancement, which originates primarily from the epicardium, sparing the subendocardial layer. - The subepicardial location is clearly distinguishable from the transmural or subendocardial delayed enhancement of ischemic necrosis.
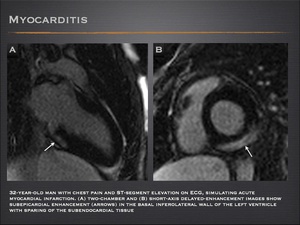
Fig.: Myocarditis
- Some patients have less severe forms of myocarditis that do not cause enough permanent injury to be detectable by delayed contrast enhancement; nonetheless they can be identified using T2-weighted MRI for edema or inflammatory changes on early (2-4 min) postcontrast T1-weighted images.
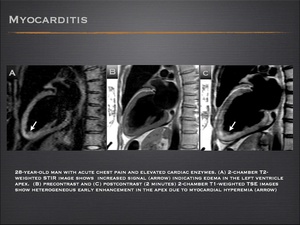
Fig.: Myocarditis
- Acute pericarditis is often accompanied by some degree of myocarditis. Myopericarditis occurs in the presence of pericardial and superficial epicardial inflammation. The myocardial injury resulting from the epicardial irritation is manifested by a number of electrocardiographic findings.
- MRI provide excellent delineation of the pericardial abnormalities caused by pericarditis, including effusion and pericardial thickening. Delayed-enhancement MRI usually shows subepicardial myocardial involvement.
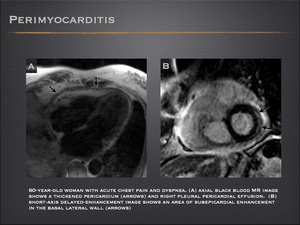
Fig.: Perimyocarditis
Cardiomyopathies
Hypertrophic cardiomyopathy (HCM)
- Chest pain is one of the major symptoms in patients with HCM. A significant percentage of these patients present with atypical chest pain and the ECG abnormalities suggest ischemia.
- Apical hypertrophic cardiomyopathy is occasionally missed by conventional echocardiography. Cardiac MRI is not subject to acoustic-window limitations and provides excellent delineation of the apical region.
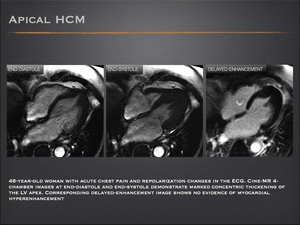
Fig.: Apical hypertrophic cardiomyopathy
- Mid-ventricular HCM is a rare form of hypertrophic cardiomyopathy that is often accompanied by an apical aneurysm. There may be associated chest pain suggestive of myocardial ischemia.
- It has been suggested that apical aneurysm may be secondary to small-vessel disease with decreased coronary flow reserve, or to the increased afterload and high apical pressure arising from the mid-ventricular obstruction.
- MRI demonstrates an hourglass appearance of the left ventricle with an aneurysm at the apex.
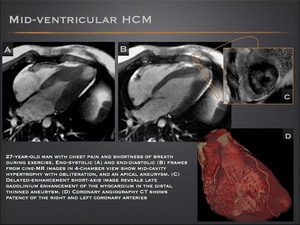
Fig.: Mid-ventricular hypertrophic cardiomyopathy
- In a small percentage of HCM patients, the heart disease progresses to the end-stage or “burned-out” phase, characterized by LV wall thinning, cavity enlargement, and systolic dysfunction.
- In this stage of the disease, the ventricular wall becomes thinner with progressive myocardial fibrous transformation, thought to be due to small-vessel ischemia.
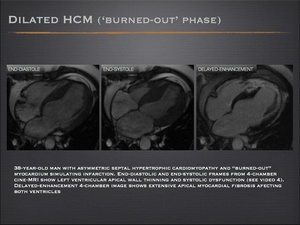
Fig.: Hypertrophic cardiomyopathy
- The MRI appearance of localized “burned out phase” forms may mimic myocardial infarction with angiographically normal coronary arteries.
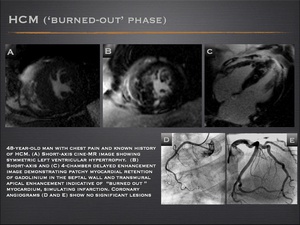
Fig.: Hypertrophic cardiomyopathy
Tako-tsubo cardiomyopathy
- Tako-tsubo cardiomyopathy is characterized by transient LV dysfunction, electrocardiographic changes that can mimic acute myocardial infarction, and release of myocardial enzymes, in the absence of obstructive coronary artery disease
- Several pathophysiological mechanisms have been proposed, but the precise etiology of this syndrome remain unknown.
- During the acute phase moderate-to-severe mid-ventricular dysfunction and apical akinesis or dyskinesis are typical, with the basal function preserved or hyperkinetic. Over a short period of days , patients usually show an considerable improvement in LV function.
- Cardiac MRI demonstrates absence of myocardial scar or infarction.
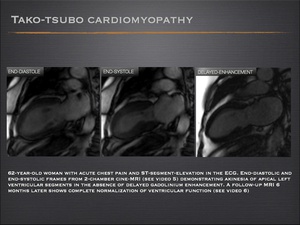
Fig.: Tako-tsubo cardiomyopathy
-
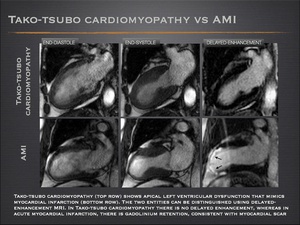
Fig.
Löffler endocarditis
- Löffler endocarditis, a kind of myositis, is one of the two forms of hypereosinophilic syndrome.
- Löffler endocarditis can present with acute chest pain with ST-segment depression on the ECG that can simulate acute myocardial infarction with normal coronary arteries.
- On biopsy, the histological findings are characterized by thickened endocardium associated with significant eosinophilic infiltration. Mural thrombi may develop in one or both ventricles.
- After administration of prednisolone, the patient’s condition and heart abnormalities improve dramatically.
- Cardiac MRI findings include thickening of the apex of one or both ventricles with extensive subendocardial delayed contrast enhancement of myocardial fibrosis. MRI can be of diagnostic assistance when a ventricular thrombus is suspected.
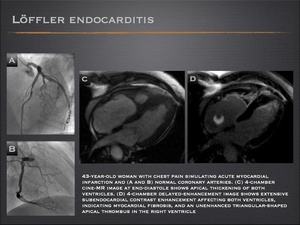
Fig.: Löffler endocarditis
Acute aortic syndrome
Acute aortic syndrome includes aortic dissection, intramural hematoma and penetrating ulcer.
Aortic dissection
- Aortic dissection is defined as a separation of the aortic layers and the presence of extraluminal blood within the layers of the aortic wall.
- The diagnosis of aortic dissection is based on demonstration of the intimal flap that separates the true from the false lumen.
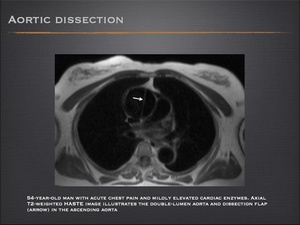
Fig.: Aortic dissection
Acute intramural hematoma
- Acute intramural hematoma is initiated by a vasa vasorum hemorrhage into the media or a penetrating atherosclerotic ulcer. The greater contrast among tissues offered by MR enables detection of small intramural hematomas, which may go unnoticed by CT.
- The typical MR finding is wall thickening with a hyperintense signal on T1- and T2-weighted images which, with fat suppression, are useful to differentiate periaortic fat from intramural hematoma.
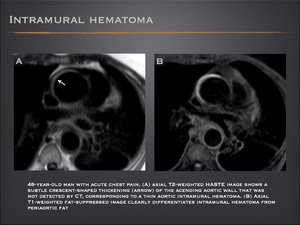
Fig.: Intramural hematoma
Penetrating ulcer
- Penetrating ulcer is an ulcerating atherosclerotic lesion that penetrates the elastic lamina and can lead to intramural hematoma or aortic rupture.
- The differential diagnosis should be established with a ulcer-like image that develops from localized dissection of an intramural hematoma and appears as a pseudoaneurysm.
Summary of findings
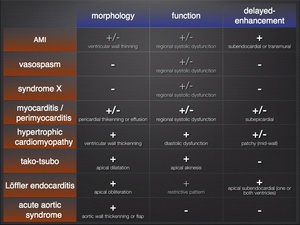
Fig.: Summary of findings table
Diagnostic algorithm
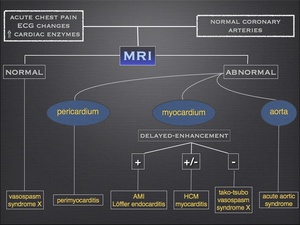
Fig.: Diagnostic algorithm
