Anatomy
Figure 1 shows an anatomical image of the foot. The midfoot includes the navicular, cuboid, and three cuneiform bones as well as the midtarsal and TMT joints. The tarsal bones are arranged in a proximal and distal row. The cuboid occupies space in both rows. The proximal row contains the navicular and the cuboid. The distal row contains the medial, intermediate, and lateral cuneiforms and the cuboid. Between the mid and forefoot there are five TMT joints. There are also multiple joints within the midfoot itself. Proximally, the three cuneiforms articulate with the navicular bone.
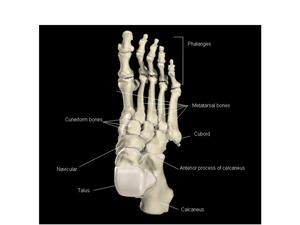
Fig.: Fig. 1
The Lisfranc joint or tarsometatarsal articulation (Figures 2a&b) consists of the bases of the 5 metatarsals, the medial, middle and lateral cuneiforms and the cuboid. The joints are bound by thick plantar ligaments extending between the tarsal and metatarsal bones 2-5, with reinforcement by attachments of the posterior tibialis tendon. The first TMT joint also has strong plantar ligaments, but is reinforced by attachments of the anterior tibialis and peroneus longus tendon. While the metatarsal bases 2-5 are linked by intermetatarsal ligaments, no such ligament exists between the 1st and 2nd metatarsal bases, with a greater risk of divergence at this site. The 2nd MT base is located between the medial and lateral cuneiform in a keystone conformation giving stability to the Lisfranc joint. The Lisfranc ligament is a strong and thick plantar ligament with relatively broad proximal attachment to the plantar surface of the medial cuneiform adjacent to the first tarsometatarsal articulation. From this attachment the ligament runs obliquely and laterally to attach to the medial aspect of the base of the second metatarsal (Fig 2c). The ligament blends partially with the capsules of the first and second tarsometatarsal joints.
Rupture of the Lisfranc ligament usually results in a midfoot disruption. This is a serious injury, leading to loss of the medial longitudinal arch and a weak midfoot.

Fig.: Fig. 2 Anatomical images show the dorsal and plantar aspects of the foot respectively.(a,b) The blue arrows show the Lisfranc ligament deep within the joint space.

Fig.: Fig. 2c Plain radiograph which shows the orientation of the Lisfranc ligament which originates from the medial cuneiform and then attaches to the base of the second metatarsal.
The arches of the foot
The foot is responsible for weight bearing and propulsion. These functions require a high degree of stability. The multiple bones and joints of the foot give it pliability in order to adapt to standing and walking on uneven surfaces however, such a segmented structure cannot bear weight unless the segments are arranged in the form of an arch (Fig. 3). The foot has a medial longitudinal arch which is higher than the lateral longitudinal arch and is composed of the calcaneus, talus, navicular, cuneiforms and the first three metatarsals. The talus occupies the highest point of the arch. The lateral longitudinal arch is lower and flatter than the medial arch and is composed of the calcaneus, cuboid, and the fourth and fifth metatarsals. There are a series of transverse arches composed of the cuneiforms, the cuboid, and the five metatarsal bases. The arches of the foot are maintained by the contours of the bones and the ligaments and muscles.

Fig.: Fig.3 Arches of the foot
Accessory bones
Accessory bones of the foot may mimic a fracture. However, they are recognised by their site, shape and smooth borders (Fig. 4).
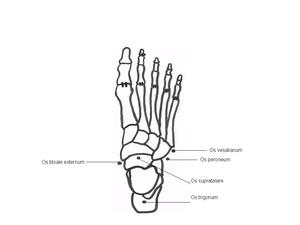
Fig.: Fig. 4 The commonest accessory bones in the foot.
Foot radiographs
AP and oblique views are performed to assess the foot.
On the AP view the medial margin of the base of the second metatarsal should align with the medial margin of the medial cuneiform (Fig. 5a). On the oblique view the medial margin of the base of the third metatarsal should align with the medial margin of the lateral cuneiform (Fig. 5b). There is overlap of several of the tarsal bones with the bases of the metatarsals on the AP radiograph of the foot.

Fig.: Fig. 5 AP and Oblique view radiographs. (a, b) The dashed red lines show the normal alignment at the Lisfranc joints.
Pitfall: it is important to perform adequate views to assess mid-foot alignment
Mid-foot fractures and dislocations
Tarsal fractures and dislocations are uncommon and usually occur as a result of severe trauma.
Talonavicular dislocation
Complex talonavicular dislocation is a rare injury. Figure 6 shows plain radiographs and CT images of complete dislocation of the talus at the talonavicular joint.
There is usually severe injury to the plantar ligamentous structures. Very often the strong 'Spring ligament' otherwise known as the plantar calcaneonavicular ligament is injured. The mechanism of injury is plantar flexion and inversion of the foot.
Treatment: surgical repair is the desired treatment.
Talar injuries with subtalar dislocation are associated with a 40% to 50% rate of AVN of the talus.
Pitfall; be sure to assess talonavicular alignment

Fig.: Fig. 6 (a,b,c,d) Plain radiographs of the ankle and foot show there is complete dislocation of the talus at the talonavicular joint, with the talar head displaced laterally so that it lies dorsal to the cuboid (dashed blue arrows). Subluxation of the calcaneocuboid joint and several small navicular fracture fragments noted.
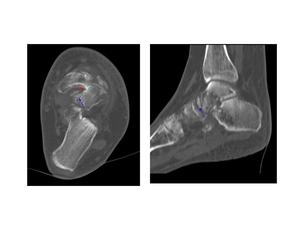
Fig.: Fig. 6 (e,f) Axial and sagittal CT images of the same patient as above show there is complete dislocation of the talus at the talonavicular joint, with the talar head displaced laterally (dashed red arrow). Several fracture fragments are seen adjacent to the talus medially and anteriorly (blue arrows).
Navicular fracture
Figure 7 shows an anatomical image and MR image of the navicular. Fractures are divided into:
- stress fracture (middle third of the navicular)
- body fracture
- cortical avulsion fracture (at insertion of tibialis posterior)
- tuberosity fracture

Fig.: Fig. 7 Anatomical image and sagittal MRI. (a,b) The dashed red arrows show the navicular bone.
Navicular stress fracture
Athletes who sustain a navicular stress fracture commonly complain of vague midfoot pain worse with activity. Relatively poor blood supply and mechanical load are two factors contributing to a significant risk of non-union.
Radiographs: often negative for stress fractures.
CT: coronal and axial CT useful if a stress fracture is suspected.
Treatment: non-weightbearing cast for 6-8 weeks until the navicular is non tender to percussion on the 'Nspot'. May take 6 months to heal, internal fixation and bone grafting is required if not improving.
Navicular body fracture
May be associated with mid-tarsal joint injuries. May occur in the coronal plane or sagittal plane (Fig.8) with displacement of the foot in a medial or lateral direction.
Body fractures can be graded:
Type I: Transverse and dorsal fragment
Type II: Transverse from dorsolateral to plantar medial across the body
Type III: Central or lateral comminution
Radiograph: the lateral projection only may show the navicular body fracture.
Treatment:
Non operative- If fracture is undisplaced, treated with a below knee walking cast.
Operative- Even if minimally displaced closed treatment not desirable as recurrent displacement of the fragments usually occurs.
Late arthritis is common.
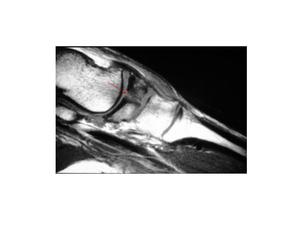
Fig.: Fig. 8 Sagittal T1 weighted MRI shows a fracture through the body of the navicular(red arrow).
Cortical avulsion and fracture of the tuberosity of the navicular
Most common type of navicular fracture due to an eversion injury to the foot as a result of tension on the posterior tibial tendon or the anterior fibres of the deltoid ligament (make sure it is not an accessory navicular). Often occurs with a compression fracture of the cuboid.
Radiograph: best viewed on AP and medial-oblique x-rays of foot in equines.
Treatment: small avulsion fractures: treated with short leg cast for 4-6 weeks.
Larger avulsion fractures: can be treated with internal fixation.
MR is the best imaging tool for all navicular fractures in particular stress fractures. It is also useful to distinguish a tuberosity fracture from an accessory navicular.
Complications:
-Arthritis
-Non-union
Pitfall: Accessory Navicular
Os tibiale externum is an accessory bone/sesamoid of tibialis posterior tendon.
Clinical issues:
Can cause medial navicular pain. MRI may show hyperintense marrow oedema on a fat suppressed T2 Weighted image.
Treatment:
Conservative: orthotic, shoe modifications.
Surgical: Kidner operation to remove the accessory navicular with reinsertion of the tibialis posterior.
Cuboid fracture
Figure 9 shows anatomical images of the cuboid bone. Isolated cuboid fractures occur due to direct trauma (Figs. 10&11). Figure 12 shows a comminuted fracture of the lateral aspect of the cuboid in a patient with early denervation arthropathy. Most cuboid fractures occur in conjunction with other fractures of the foot. Nutcracker injury occurs as a result of compression between the calcaneus and 4th and 5th metatarsals and can be associated with a midfoot fracture and Lisfranc fracture.
Treatment: In order to re-establish the length of the lateral column of the foot, bone grafting and internal fixation is required.
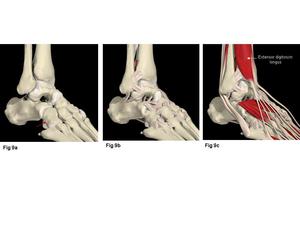
Fig.: Fig. 9a Anatomical model showing articulations of the cuboid (red arrow) with the bases of the 4th and 5th metatarsals. Fig. 9b shows the tarsal and tarsometatarsal ligaments. Fig. 9c shows the extensor digitorum brevis and hallucis tendons overlying the dorsum of the foot.

Fig.: Fig. 10 AP and oblique radiographs of the right foot. (a,b) Show a small undisplaced fracture (blue arrow) involving the lateral margin of the cuboid.

Fig.: Fig 11 a, b. Plain radiographs show a fracture at the lateral margin of the cuboid (red arrow).

Fig.: Fig. 11 CT images in the same patient as above. (c,d) The red arrow shows the fracture fragment.

Fig.: Fig. 12 Plain radiograph and CT image. (a,b) There is a fracture of the cuboid in a patient with early denervation arthropathy, extending into the calcaneocuboid joint denoted by the dashed red arrow.
Cuneiform fracture
Cuneiform fractures can occur in isolation but generally occur in conjunction with other fractures of the midfoot (Fig. 13). In particular, the Lisfranc dislocation is often associated with cuneiform fractures (Fig.14). The mechanism of injury for these fractures is usually from an axial load through the foot, though direct crushing forces on the midfoot can also cause these fractures.

Fig.: Fig. 13 Radiograph and coronal CT. (a,b) Fractured distal aspects lateral cuneiform and 4th metatarsal.

Fig.: Fig.14 Plain radiographs. (a,b) Show a fractured medial cuneiform with awidened gap between the 1st and 2nd metatarsal bases (dashed blue arrow).

Fig.: Fig. 14 T1 and T2 weighted MRI images in the same patient as above. (c,d) Fractured medial cuneiform (red arrows), widened gap between bases of 1st and 2nd metatarsals. The Lisfranc ligament is not seen and is possibly avulsed and attached to the medial cuneiform fracture fragment.
Lisfranc injury
Jacques Lisfranc (1790-1847) was a field surgeon in Napoleon's army described an amputation through the tarsometatarsal joint to treat gangrene of the foot after a soldier suffered an injury following a fall from his horse with his foot caught in the stirrup. The injury occurs when there is a dislocation or fracture and dislocation between the forefoot and midfoot (Figures 15&16). The Lisfranc injury occurs due to an injury to the ligaments that connect these joints.

Fig.: Fig. 15a Plain radiographs show a Lisfranc injury (refer to table 1). There is widening between the bases of the 1st and 2nd metatarsals (dashed red arrow) and an oblique fracture of the neck of the fifth metatarsal.Fig. 15b Corresponding CT image shows widening between the bases of the 1st and 2nd metatarsals (blue dashed arrow). There are fractures at the bases of the 2nd and 3rd metatarsals as well as the neck of the 2nd metatarsal.

Fig.: Fig. 16 Plain radiographs and CT reconstruction of a Lisfranc injury to the left foot. There is widening between the bases of the 1st and 2nd metatarsals (dashed red arrows). There are fractures at the bases of the 2nd,3rd and 4th metatarsals.
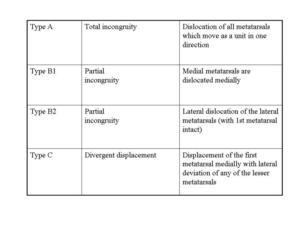
Fig.: Classification of Lisfranc Injuries
Imaging
The Lisfranc injury is uncommon, accounting for approximately 1% of all fractures.
However, up to 20% of these injuries are missed on conventional AP and oblique radiographs.
CT:when acquired parallel to the long axis of the metatarsals may show malalignments and fractures not clearly seen on conventional radiographs.
MRI: has the advantage of lack of ionising radiation and good soft tissue delineation in multiple planes. MRI shows disruption to the Lisfranc ligament (Fig. 17) as well as other ligamentous damage, local soft tissue and marrow oedema. It is a useful tool in surgical planning. Tears of the Lisfranc ligament may be partial or complete, with partial tears usually involving the weaker dorsal band.
Treatment:conventionally, conservative management of these injuries in non-weight bearing casts was the treatment of choice. However, this often resulted in permanent ligamentous laxity or disruption with consequent foot instability, severe arthritis or even Sudek's atrophy. Current imaging techniques of CT and MRI allows early diagnosis of both bony and soft tissue injury. Closed reduction with percutaneous pinning or open reduction with internal fixation may be used, the choice of treatment depending on the degree of angulation and displacement of bones and any associated fractures. Undisplaced unstable injuries should be treated with percutaneous wire fixation (Fig. 18), and displaced or angulated injuries are often treated with cannulated screws. Primary fusion is recommended for purely ligamentous injuries or injuries with severe articular damage.

Fig.: Fig. 17 T2 fat sat axial MRI images. (a,b) Showing avulsion of the Lisfranc ligament (red arrow) from the medial cuneiform with surrounding oedema and a joint effusion.

Fig.: Fig. 18 Percutaneous wire fixation of a Lisfranc injury.
Complications of midfoot fractures and dislocations:
- Compartment syndrome: Can occur following trauma, surgery or repetitive and extensive muscle use. Increased pressure within a confined fascial compartment impairs blood supply which can cause ischaemia of the muscles and nerves leading to eventual irreversible damage and death of the tissues without prompt treatment.
- Ischaemia/ Avascular necrosis (Fig. 19)
- Neurological compromise/ Charcot's arthropathy
- Osteoarthritis (Fig. 20)

Fig.: Fig. 19 Avascular necrosis (AVN) of the Navicular.

Fig.: Fig. 20 Long standing fracture of the base of the 2nd metatarsal with osteophyte and subchondral cyst formation.
Pitfalls:
1. Imaging: AP/oblique radiograph orientation.
2. Accessory Ossicles - can be normal
- may have bone marrow oedema/ fracture
