Introduction
Carcinoid tumors originate in the enterochromaffin cells and belong to the apudoma category of tumors. They arise from the Kulchitsky cells in the crypts of Lieberkühn and grow as submucosal nodules. Carcinoid tumors are uncommon neuroendocrine tumors; their overall incidence is 1.9/100,000.
They most commonly occur in the gastrointestinal tract (66%), predominantly in the small bowel (42%). They can also occur in the pancreas, lung, and ovary.
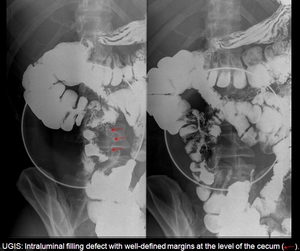
Fig.: UGIS
Carcinoid tumors grow slowly for years. Patients usually remain asymptomatic until the tumor is very large or has metastasized, especially to the liver and bone. The probability of metastasis is related with the size of the tumor.
Carcinoid tumors can secrete vasoactive substances like 5-hydroxytryptamine, tachykinins, kallikrein, histamine, adrenocorticotropic hormone, gastrin, calcitonin, growth hormone, prostaglandins, and others, which tend to be deactivated through a series of reactions and processes when they pass through the liver.
The carcinoid syndrome occurs when the tumor has metastasized to the liver and the above-mentioned substances reach the systemic circulation through the hepatic vein before they can be deactivated. It manifests clinically as diarrhea, bronchospasm, palpitations, and flushing.
The vasoactive substances secreted from the liver by the metastatic tumor cells reach the right heart through the inferior vena cava, and may cause involvement of the heart, referred to as carcinoid heart syndrome (CHS).
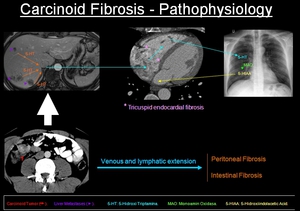
Fig.: Pathophysiology
Between 20% and 50% of patients with carcinoid syndrome develop CHS. There is a slight male predominance (60%) and the mean age at diagnosis is 56 to 63 years.
Exceptionally, carcinoid tumors without liver metastases also cause CHS (some tumors in the ovaries, lungs, and the retroperitoneal lymph nodes metastases) because the vasoactive substances pass directly into the systemic circulation without passing through the liver through ovarian, pulmonary, and retroperitoneal veins, respectively.
Pathogenesis
The pathogenesis of CHS is poorly understood. Different studies point to a fundamental role for 5-hydroxytryptamine or serotonin, because they regulate the synthesis of tissue growth factor beta, which accumulates in the heart valves of patients with CHS and stimulates collagen formation by the interstitial cells of the heart valves.
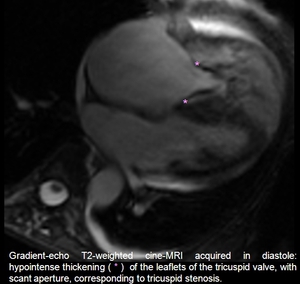
Fig.: MRI 4C
5-hydroxytryptamine is metabolized by monoamine oxidases in the liver, lungs, and brain into 5-hydroxyindole-3-acetic acid (5-HIAA), a metabolite that has been shown to induce cardiac fibrosis and valvular disease in animals. The tachykinins, neuropeptide K, substance P, and the N-terminal natriuretic brain peptides have also been implicated.
Another theory is that these substances damage the endocardium, and attempts at healing cause increased permeability of the vascular endothelium and lead to an excess of fibroblastic proliferation and mural thrombosis.
Histological study
Macroscopic examination reveals wall thickening, shortening of the valves and tendinous cords, and a pearl-white color. The morphology of the valve remains intact with an overlying layer of fibrous tissue at the level of the endocardium. The subvalvular apparatus, including the tendinous cords and the papillary muscles, is also affected.
There is a proliferation of myofibroblasts with collagen deposits in all the plaques, as well as the development of a myxoid matrix (98%), neovascularization (94%), inflammation (94%), and elastosis (20%).
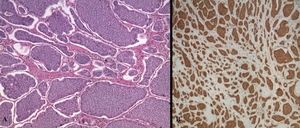
Fig.: Hematoxylin-eosin staining (A) and Immunohistochemical staining for EGFR (B) show proliferation of myofibroblasts with collagen deposits, as well as the development of a myxoid matrix, neovascularization, and elastosis.
Clinical presentation
Characteristically, the right heart is involved. The tricuspid is the valve most commonly affected in CHS; tricuspid involvement usually manifests as regurgitation. The tricuspid valve plaques tend to develop on the ventricular side of the leaflets, causing adhesions in the endocardial wall and favoring regurgitation. The fibrous tissue in the valvular ring causes constriction, resulting in a certain degree of valvular stenosis.
In the pulmonary valve, the predominant lesion is stenosis because the plaques develop in the root of the pulmonary artery, decreasing its caliber.
In 10% of cases, the valves of the left heart are involved and angina associated to coronary vasospasm develops. Left heart valve disease tends to occur in cases with a patent foramen ovale or with bronchopulmonary carcinoid tumor. The sparing of the left heart can be explained by a certain degradation of the vasoactive substances in the lungs that results in their reaching the pulmonary veins, left atrium, and left ventricle in an inactive state.
Metastases to the heart are rare (<5%) and they are believed to be caused by processes unrelated to the substances secreted.
Diagnosis
It is important to consider CHS in the diagnosis of patients with carcinoid tumors, especially if they have liver metastases.

Fig.: Abdominal US
The clinical presentation is often subtle, even in advanced stages of disease, but right heart failure eventually occurs.
At physical examination, pansystolic valvular murmurs (tricuspid regurgitation and pulmonary stenosis), early diastolic murmur (pulmonary artery regurgitation), and jugular engorgement are present, as well as symptoms of right heart failure like dyspnea, peripheral edema, hepatomegaly, and ascites as the disease progresses.
The ECG is normal in 50% of cases, although the alterations caused by CHS show a P pulmonale due to pulmonary hypotension and right atrial hypertrophy, sinus tachycardia, ventricular fibrillation, hypovoltage of the QRS complex, nonspecific changes in the ST segment, and right branch block.
Once CHS has been suspected, we should proceed to directed imaging tests, fundamentally echocardiography, cardiac MRI, and cardiac CT.
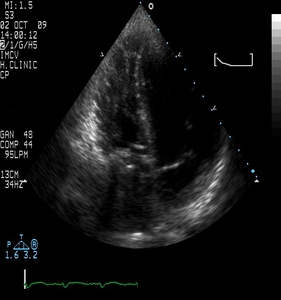
Fig.: 4 chamber view echocardiography, showing a thickening and irregularity of the tricuspid valve.
Differential diagnosis
Some entities can present similar alterations. The main differential diagnosis is with rheumatic heart disease, which rarely affects only the right heart.
Other causes of acquired tricuspid valve disease include prolapse, bacterial endocarditis, rupture of the papillary muscle, and some cardiac tumors.
Drugs used for weight loss, like fentfluramine and phentermine, can also cause valvular disease due to their serotonergic effects. Dopaminergic agonists derived from ergotamine, like pergolide, bromocriptine, cabergoline, and methysergide can also affect the heart.
Treatment
Treatment of carcinoid syndrome is aimed at slowing progression and treating symptoms rather than curing the disease itself. It is based on somatostatin analogues. Surgery has an important role, especially in nondisseminated tumors.
Liver metastases can also be treated surgically or percutaneously with radiofrequency ablation and/or embolization, and these treatments can be combined with chemoembolization. Chemotherapy is also used occasionally, and new drugs like imatinib and endostatin might prove useful in the future.
When CHS appears, diuretics are used in cases of heart failure; digoxin is also used sometimes, together with heart valve surgery.
Follow-up
The main tumor markers used in follow-up are 5-HIAA and chromogranin A (Cg A). 5-HIAA is more specific and is associated to symptoms whereas Cg A is related to the size of the tumor. Imaging tests, including CT, MRI, nuclear medicine, and echocardiography, are also fundamental.
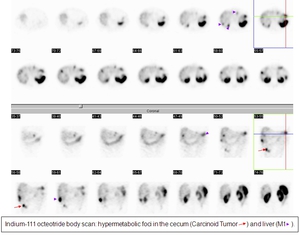
Fig.: Octreoscan: it is very useful in the monitoring.
Prognosis
When carcinoid tumors present with CHS, life expectancy is reduced from 4.6 to 1.6 years. The prognosis improves with new treatments and early diagnosis of liver metastases.
