Correlating the histologic subtypes of abdominal liposarcoma with the radiologic findings presents a clinical challenge, as there are no specific imaging features across the spectrum of subtypes. In addition, it is often difficult to use imaging findings to diagnose abdominal liposarcoma when it lacks a fat component.
Liposarcoma lesions sometimes include multiple histologic subtypes; thus variable CT attenuation or MR signal intensity may be found within the same lesion. Such histologic subtypes are usually classified on the basis of the most aggressive cellular component.
The imaging findings for the tumors that have one or two histologic subtype components appear to be a combination of the characteristic findings for the individual subtypes.
Well-differentiated Liposarcoma
Well-differentiated liposarcoma contains mature fatty elements with imaging characteristics that may be indistinguishable from those of normal fat, leading frequently to the erroneous diagnosis of lipoma. Lipomas rarely occur in the retroperitoneum, and fat-containing lesions in this location should never be dismissed as benign lipoma, even if the mass presents with very suggestive imaging features. A cautious approach should be adopted and the lesion considered a well-differentiated liposarcoma and treated as so until further characterization.
Imaging features that favor well-differentiated liposarcoma over lipoma include large lesion size (> 10 cm), presence of thick septa (> 2 mm), nodular or globular areas, nonadipose mass-like areas within the lesion, and decreased percentage of fat composition (< 75% fat in mass).
At CT, the lesions demonstrate fat attenuation [Fig. 1; Fig. 2-3]. On T1-weighted imaging (T1-WI) and T2-weighted imaging (T2-WI), well-differentiated liposarcomas are usually isointense to subcutaneous fat, with loss of signal intensity (SI) on fat-suppressed imaging sequences [Fig. 2-3; Fig. 4].

Fig.: (1) Well-differentiated liposarcoma in a 58 year-old patient. Contrast-enhanced CT scan reveals a huge fatty mass that displaces the abdominal contents to the right and causes left hydronephrosis. Multiple coarse, thickened septa of soft tissue attenuation (arrowheads) are present in the mass and suggest the diagnosis of liposarcoma. A solid-appearing area of ill-defined margins and non-fatty attenuation is also noted and better depicted on the coronal reformation (arrows).

Fig.: (2) CT and MR illustration of a well-differentiated liposarcoma in a 69 year-old patient with a history of gastric GIST. Unenhanced CT image (A) reveals a relatively well-defined lipomatous mass in the left iliac fossa. The lesion displays central calcifications (arrowhead), as well as few internal septations and fibrous strands. Axial T1-WI (B) and T2-WI (C) show the mass to be isointense to subcutaneous fat. Marked signal loss is observed on axial fat-suppressed T2-WI (D), confirming the fatty nature of the mass.

Fig.: (3) Coronal T2-WI of the same patient as in Fig. 2 depicts the mass extending from the abdominal cavity to the proximal thigh region.

Fig.: (4) MR depiction of a pelvic well-differentiated liposarcoma in a 38 year-old woman. Unenhanced coronal T1-WI (A) and axial T2-WI (B) show an anterior pelvic mass isointense to subcutaneous fat. Sagital fat-suppressed T1-WI (C) demonstrates homogeneous signal loss throughout the lesion. Some thin internal septations are observed after contrast administration (D), but there are no nodular enhancing areas. During surgical resection, the mass was found to originate from the mesosigmoid.
Well-differentiated liposarcomas are usually round or lobulated, displacing or surrounding normal structures. They frequently contain septa, as well as occasional nonadipose, solid-appearing regions [Fig. 5-6; Fig. 7]. These nonfatty areas are isointense relative to skeletal muscle on T1-weighted images and iso- to hyperintense on T2-weighted images. The solid-appearing regions can be poorly defined, with no clear demarcation between them and fat [Fig. 1]. After administration of contrast material, the solid areas usually enhance [Fig. 5; Fig. 7].
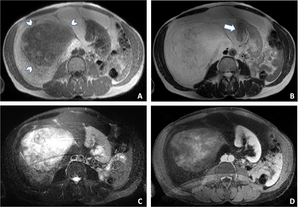
Fig.: (5) MR depiction of a well-differentiated liposarcoma with lipoma-like and myxoid components in a 52 year-old woman. Axial T1-WI (A) and T2-WI (B) show a large right retroperitoneal mass that is isointense to subcutaneous fat and displaces the abdominal structures to the left, including the right kidney (arrow). A round area of myxoid component (arrowheads, A) is observed infiltrating the lipoma-like component and appears to be isointense to skeletal muscle. Axial fat-suppressed T2-WI (C) shows low SI of the suppressed lipoma-like components of the tumor and a higher SI within the myxoid portion. Axial fat-suppressed contrast-enhanced T1-WI (D) reveals heterogeneous enhancement of the nonfatty portion of the mass.

Fig.: (6) Coronal T2-WI of the same patient as in Fig. 5 improves the definition of the craniocaudal extent of the huge sarcomatous mass and shows to better advantage the extrinsic mass effect on the liver and displacement of virtually all the major retroperitoneal structures.

Fig.: (7) Well-differentiated liposarcoma with extensive nonfatty elements in a 56 year-old man. Axial unenhanced CT images (A-B) reveal a large ill-defined abdominal mass of predominantly fat attenuation that engulfs the left kidney and displaces the abdominal contents to the contralateral side. Central calcifications are also present. Several nodular higher attenuation areas (arrowheads, B) are noted within the mass, corresponding to a dedifferentiated component. The solid areas show mild heterogeneous enhancement in the late phase of contrast administration (C-D). The patient was submitted to surgical resection of the tumor with concomitant left nephrectomy, hemicolectomy and splenectomy.
Dedifferentiated Liposarcoma
Histologically, dedifferentiated liposarcomas have areas of well-differentiated liposarcoma and a nonfatty (dedifferentiated) component, corresponding on imaging studies to solid, well demarcated lesions, with distinct planes between fat and solid tumor [Fig. 8; Fig. 9].
Calcifications or ossification within a liposarcoma may be a sign of dedifferentiation [Fig. 8; Fig. 10].

Fig.: (8) CT and MR illustration of a dedifferentiated liposarcoma in a 30 year-old woman. Axial contrast enhanced CT image (A) shows two relatively well demarcated nonfatty nodular lesions (arrows) in the proximity of the pancreatic head and anterior to the splenic vessels. One of the nodules displays some coarse calcifications (arrowheads, A-B). A well-differentiated tumor portion with fatty density is observed on the coronal CT image (*, B). The nonfatty nodular lesions reveal low SI on unenhanced T1-weighted MR imaging (C) and an heterogeneous enhancement pattern after gadolinium administration (D).

Fig.: (9) Enhanced axial CT scan of a dedifferentiated liposarcoma in a 57 year-old man, revealing two distinct nodular posterior lipomatous and anterior nonfatty components.

Fig.: (10) CT depiction of a dedifferentiated liposarcoma in a 75 year-old man. Axial unenhanced CT scans reveal a very large heterogeneous retroperitoneal mass that extends from the inferior hepatic border to the pelvic inlet. Multiple coarsely calcified areas (arrowheads) are embedded within the tumor. The mass contacts and displaces several abdominal structures, including pancreas, right kidney and major retroperitoneal vessels.
On MR, the mass-like areas of nonfatty tissue predominate over the fat-containing well-differentiated tumor, revealing low T1-WI and high T2-WI SI [Fig. 8; Fig. 11-12].

Fig.: (11) Dedifferentiated liposarcoma in a 43 year-old woman. MR imaging shows a left retroperitoneal and anterior abdominal mass of predominantely nonfatty SI, with low SI on T1-WI (A) and areas of high SI on T2-WI (B). Fat-suppressed T1-WI (C) obtained after contrast administration demonstrates heterogeneous peripheral enhancement of the lesion.

Fig.: (12) Coronal T2-WI of the same patient as in Fig. 11 shows superior displacement of the left kidney (arrows).
Nevertheless, the CT attenuation, MR signal characteristics and enhancement patterns of these nonlipomatous masses are nonspecific [Fig. 13], and frequently pose a diagnostic dilemma with other types of sarcoma.

Fig.: (13) Dedifferentiated liposarcoma in a 70 year-old patient. Axial CT scan without contrast administration (A) depicts a well defined nodular mass occupying the left posterior peri-renal space. The tumor reveals heterogeneous predominantely nonfatty density. A nonspecific predominantely peripheral enhancement is seen in the late phase of contrast administration (B-C).
Myxoid Liposarcoma
Myxoid liposarcomas are composed of a myxoid matrix containing mucopolysaccharides with small amounts of mature fat. A spectrum of imaging features may be present in myxoid liposarcomas related to the fat content, amount of myxoid material, degree of cellularity and vascularity, and presence of necrosis.
At CT, they often have an inhomogeneous appearance, with CT attenuation values less than that of muscle. Occasionally, fat and soft tissue elements are distributed homogeneously within the lesion, producing fluid attenuation [Fig. 14; Fig. 15]. Consequently, the lesion may appear cystic on unenhanced CT images and cause diagnostic confusion.

Fig.: (14) Mesenteric myxoid liposarcoma with round cell component in a 68 year-old patient admitted for a suspected adnexial mass. Axial contrast-enhanced CT images show a lobulated inhomogeneous mass localized to the retroperitoneal space, with anterior displacement of bowel loops. The mass displays geographic areas of fluid attenuation owing to admixture of fatty and soft tissue components. Some enhancing septa and nodular mural components are also recognizable.

Fig.: (15) Axial contrast enhanced CT scan of a 53 year-old woman with recurrent myxoid liposarcoma. A large retroperitoneal mass with low attenuation areas is seen extending from the left hypochondrium to the pelvic inlet. The tumor displaces several abdominal structures and produces mass-effect on the posterior gastric wall (arrowheads).
At MR imaging, myxoid liposarcomas exhibit signal intensity similar to that of water: low signal intensity on unenhanced T1-WI and high signal intensity on T2-WI, although they are not isoattenuating relative to pure fluid [Fig. 5]. Thus, these malignant lesions may superficially resemble benign cysts at unenhanced MR imaging. Foci of fat or low SI septa may be revealed within the predominantly myxoid-containing mass.
The myxoid stroma will display a variable enhancement depending on its degree of vascularity, and thus enhanced images can distinguish cystic and myxoid components of these tumors [Fig. 14].
Pleomorphic Liposarcoma
Pleomorphic liposarcoma is the least common subtype of retroperitoneal liposarcoma. Histologically, there is a disorderly growth pattern with a marked degree of cellular pleomorphism, giving rise to heterogeneous nonfatty tumors with imaging characteristics indistinguishable from those of other malignant soft-tissue masses. Mature fat may not be radiologically visible within the lesion. Necrosis and hemorrhage may cause MR signal heterogeneity and nonenhancing areas.

 Well-differentiated liposarcoma in a 58 year-old patient. Contrast-enhanced CT scan reveals a huge fatty mass that displaces the abdominal contents to the right and causes left hydronephrosis. Multiple coarse, thickened septa of soft tissue attenuation (arrowheads) are present in the mass and suggest the diagnosis of liposarcoma. A solid-appearing area of ill-defined margins and non-fatty attenuation is also noted and better depicted on the coronal reformation (arrows).")
 CT and MR illustration of a well-differentiated liposarcoma in a 69 year-old patient with a history of gastric GIST. Unenhanced CT image (A) reveals a relatively well-defined lipomatous mass in the left iliac fossa. The lesion displays central calcifications (arrowhead), as well as few internal septations and fibrous strands. Axial T1-WI (B) and T2-WI (C) show the mass to be isointense to subcutaneous fat. Marked signal loss is observed on axial fat-suppressed T2-WI (D), confirming the fatty nature of the mass.")
 Coronal T2-WI of the same patient as in Fig. 2 depicts the mass extending from the abdominal cavity to the proximal thigh region.")
 MR depiction of a pelvic well-differentiated liposarcoma in a 38 year-old woman. Unenhanced coronal T1-WI (A) and axial T2-WI (B) show an anterior pelvic mass isointense to subcutaneous fat. Sagital fat-suppressed T1-WI (C) demonstrates homogeneous signal loss throughout the lesion. Some thin internal septations are observed after contrast administration (D), but there are no nodular enhancing areas. During surgical resection, the mass was found to originate from the mesosigmoid.")
 MR depiction of a well-differentiated liposarcoma with lipoma-like and myxoid components in a 52 year-old woman. Axial T1-WI (A) and T2-WI (B) show a large right retroperitoneal mass that is isointense to subcutaneous fat and displaces the abdominal structures to the left, including the right kidney (arrow). A round area of myxoid component (arrowheads, A) is observed infiltrating the lipoma-like component and appears to be isointense to skeletal muscle. Axial fat-suppressed T2-WI (C) shows low SI of the suppressed lipoma-like components of the tumor and a higher SI within the myxoid portion. Axial fat-suppressed contrast-enhanced T1-WI (D) reveals heterogeneous enhancement of the nonfatty portion of the mass.")
 Coronal T2-WI of the same patient as in Fig. 5 improves the definition of the craniocaudal extent of the huge sarcomatous mass and shows to better advantage the extrinsic mass effect on the liver and displacement of virtually all the major retroperitoneal structures.")
 Well-differentiated liposarcoma with extensive nonfatty elements in a 56 year-old man. Axial unenhanced CT images (A-B) reveal a large ill-defined abdominal mass of predominantly fat attenuation that engulfs the left kidney and displaces the abdominal contents to the contralateral side. Central calcifications are also present. Several nodular higher attenuation areas (arrowheads, B) are noted within the mass, corresponding to a dedifferentiated component. The solid areas show mild heterogeneous enhancement in the late phase of contrast administration (C-D). The patient was submitted to surgical resection of the tumor with concomitant left nephrectomy, hemicolectomy and splenectomy.")
 CT and MR illustration of a dedifferentiated liposarcoma in a 30 year-old woman. Axial contrast enhanced CT image (A) shows two relatively well demarcated nonfatty nodular lesions (arrows) in the proximity of the pancreatic head and anterior to the splenic vessels. One of the nodules displays some coarse calcifications (arrowheads, A-B). A well-differentiated tumor portion with fatty density is observed on the coronal CT image (*, B). The nonfatty nodular lesions reveal low SI on unenhanced T1-weighted MR imaging (C) and an heterogeneous enhancement pattern after gadolinium administration (D).")
 Enhanced axial CT scan of a dedifferentiated liposarcoma in a 57 year-old man, revealing two distinct nodular posterior lipomatous and anterior nonfatty components.")
 CT depiction of a dedifferentiated liposarcoma in a 75 year-old man. Axial unenhanced CT scans reveal a very large heterogeneous retroperitoneal mass that extends from the inferior hepatic border to the pelvic inlet. Multiple coarsely calcified areas (arrowheads) are embedded within the tumor. The mass contacts and displaces several abdominal structures, including pancreas, right kidney and major retroperitoneal vessels.")
 Dedifferentiated liposarcoma in a 43 year-old woman. MR imaging shows a left retroperitoneal and anterior abdominal mass of predominantely nonfatty SI, with low SI on T1-WI (A) and areas of high SI on T2-WI (B). Fat-suppressed T1-WI (C) obtained after contrast administration demonstrates heterogeneous peripheral enhancement of the lesion.")
 Coronal T2-WI of the same patient as in Fig. 11 shows superior displacement of the left kidney (arrows).")
 Dedifferentiated liposarcoma in a 70 year-old patient. Axial CT scan without contrast administration (A) depicts a well defined nodular mass occupying the left posterior peri-renal space. The tumor reveals heterogeneous predominantely nonfatty density. A nonspecific predominantely peripheral enhancement is seen in the late phase of contrast administration (B-C).")
 Mesenteric myxoid liposarcoma with round cell component in a 68 year-old patient admitted for a suspected adnexial mass. Axial contrast-enhanced CT images show a lobulated inhomogeneous mass localized to the retroperitoneal space, with anterior displacement of bowel loops. The mass displays geographic areas of fluid attenuation owing to admixture of fatty and soft tissue components. Some enhancing septa and nodular mural components are also recognizable.")
 Axial contrast enhanced CT scan of a 53 year-old woman with recurrent myxoid liposarcoma. A large retroperitoneal mass with low attenuation areas is seen extending from the left hypochondrium to the pelvic inlet. The tumor displaces several abdominal structures and produces mass-effect on the posterior gastric wall (arrowheads).")