The first scan was performed on an axial plane at the apex of the Scarpa’s triangle, where the sartorius muscle crosses anteriorly the superficial femoral artery. The superficial femoral artery origins in the femoral triangle (Scarpa's triangle), 2 to 5 cm distally to the inguinal ligament, where the common femoral artery bifurcates originating the deep femoral artery. Then, the superficial femoral artery enters the adductors’ canal, which is in continuity with the apex of the Scarpa's triangle. The division of the common femoral artery was easily assessed on axial US scans as the superficial femoral artery is the most superficial vessel in relation with the deep fascia of the sartorius muscle (Figure1).
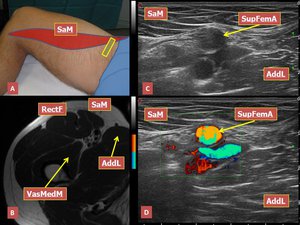
Fig.: Figure 1. A) Transducer orientation on the crural region at the apex of the femoral triangle. B) Axial MR section showing the vascular structures at the apex of the femoral triangle which is in continuity with the adductor canal. C) The deep fascia of sartorius muscle is in relation with the anterior aspect of the superficial femoral artery wall. D) Corresponding color-Doppler axial scan. Legend: SaM, sartorius muscle; SupFemA, superficial femoral artery; AddL, adductor longus muscle; RectF, rectus femoris muscle; VasMedM, vastus medialis muscle.
The posteromedial wall of the adductor canal is formed proximally by adductor longus muscle, more distally by adductor magnus muscle and these two muscles are an useful anatomical reference to divide the adductor canal in two segments. The muscular belly of adductor longus, which insertes on the middle third of the linea aspera, becomes progressively thinner caudally. Vastus medialis muscle forms the posterolateral and lateral limits; the deep muscular fascia of sartorius represents the anterior wall. In this proximal part of Hunter’s canal the saphenous nerve, which is the largest cutaneous branch of the Femoral nerve, is lateral to the superficial femoral artery and the femoral vein isposterior to the artery. The saphenous nerve was appreciable on axial US scans due to its typical "honeycomb" appearance; on longitudinal US scans the nerve revealed a fascicular echostructure (Figure 2).

Fig.: Figure 2. A) Transducer orientation on the anteromedial aspect of the thigh. B) Axial oblique US scan showing the neurovascular bundle inside the proximal third of the adductor canal. The saphenous nerve is lateral to the femoral artery; the femoral vein is posterior. The posterior wall is represented by adductor longus muscle. C) Corresponding color-Doppler axial scan showing the “honeycomb” echostructure of the saphenous nerve, adjacent to the arterial wall. Legend: SaM, sartorius muscle; SaphN, saphenous nerve; FemA, femoral artery; Fem V, femoral vein; VasMedM, vastus medialis muscle; AddL, adductor longus muscle.
In all subjects a venous vessel, originating from the medial aspect of the superficial femoral vein, was appreciable passing through the intermuscular connective space between sartorius and adductor longus muscles. This venous vessel is a tributary of the great saphenous vein and the color-Doppler module aided its detection (Figure 3).

Fig.: Figure 3. A) Transducer orientation on the medial aspect of the middle third of the thigh. B, C) Two adjacent US axial scans demonstrating the perforating venous branch emerging from the medial aspect of the superficial femoral vein to move medially toward the great saphenous vein which is located in the superficial fascia, between sartorius (anterior) and gracilis muscles (posterior). At this level the posterior wall of the adductor canal is still formed by the adductor longus muscle. D) Corresponding axial MR section showing the great saphenous vein in the superficial fascia. Legend: SaM, sartorius muscle; FemA, femoral artery; FemV, femoral vein; VasMedM, vastus medialis muscle; AddL, adductor longus muscle; PerfBGSv, perforating branch of the great saphenous vein; GSv, great saphenous vein; GraM, gracilis muscle.
At the origin of this communicating vein, the saphenous nerve is still lateral to the superficial femoral artery but more anterior (Figure 4).

Fig.: Figure 4. Axial US image at the site of origin of the perforating venous branch, tributary of the great saphenous vein. At this level the saphenous nerve is still lateral to the femoral artery. SaM, sartorius muscle; FemA, femoral artery; FemV, femoral vein; VasMedM, vastus medialis muscle; AddL, adductor longus muscle; SaphN, saphenous nerve.
Caudally the adductor longus muscle belly was still not detectable and the posterior wall of the canal is represented only by adductor magnus muscle, which was considered as the most important reference to guide the US assessment of the distal segment of the canal and of the hiatal region. It is important to remember that the adductor magnus muscle is made of two different parts, defined by the orientation of their fibers. The medial part of the adductor magnus, often called the 'hamstring part', originates from the ischial tuberosity of the pelvic bone and descends almost vertically along the thigh to insert by a rounded tendon into the adductor tubercle on the medial condyle of the distal head of the femur. The most lateral part (adductor part) inserts onto the medial supracondylar line and the medial margin of the linea aspera. The adductor hiatus is a large circular gap located inferiorly between the hamstring and adductor parts of the adductor magnus, which allows the femoral artery and associated veins to pass from the adductor canal to the popliteal fossa posterior to the knee (Figures 5, 6).
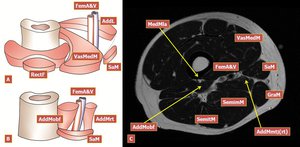
Fig.: Figure 5. A, B) Schematic drawing illustrating the boundaries of the proximal and distal parts of the Hunter’s canal. Note that adductor canal hiatus is delimited medially by the longitudinal fibers of adductor magnus muscle and its rounded tendon, laterally by the oblique fibers of adductor magnus. C) Axial MR scan showing the hamstring part (longitudinal fibers) of the adductor magnus with its myotendinous junction and the adductor part (oblique fibers) which inserts via an aponeurosis on the medial margin of the linea aspera. Legend: SaM, sartorius muscle; FemA, femoral artery; FemV, femoral vein; VasMedM, vastus medialis muscle; AddMmtj(rt), adductor magnus myotendinous junction (origin of the rounded tendon); AddMobf, oblique fibers of adductor magnus; MedMla, medial margin of linea aspera; SemimM, semimembranosus muscle; SemitM, semitendinosus muscle; GraM, gracilis muscle.
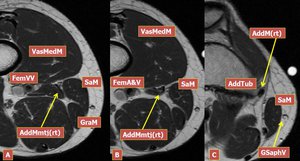
Fig.: Figure 6. A, B, C Three axial MR scans showing the myotendinous junction of the hamstring part of adductor magnus, where origins the rounded tendon. Legend: SaM, sartorius muscle; FemVV, femoral vessels; VasMedM, vastus medialis muscle; AddMmtj(rt), adductor magnus myotendinous junction (origin of the rounded tendon); GraM, gracilis muscle; GSaphV, great saphenous vein; AddTub, adductor tubercle.
In this second segment of the canal (bounded postero-medially by adductor magnus muscle) the saphenous nerve becomes progressively more anterior to the superficial femoral artery while the femoral vein becomes posterior to the artery. A slight “up and down” motion of the transducer on axial planes was helpful in detecting the peripheral nerve when it was not easily cleavable from the surrounding connective tissue of the subsartorial canal. The visualization of the perineurium as a clear hyperechoic interface was very difficult (Figure 7).
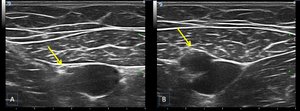
Fig.: Figure 7. A, B Two axial US scans demonstrating the course of the saphenous nerve which moves from a lateral position to the femoral artery to an anterior position to this vessel near the hiatal region. The saphenous nerve may be identified on axial US scans between the anterior surface of the arterial wall and the deep fascia of sartorius muscle Arrow, saphenous nerve.
More caudally the femoral artery and vein move progressively in a postero-lateral direction while the saphenous nerve remains anterior, in close relation to the deep fascia of the lateral extremity of sartorius muscle and the anterior wall of a small branch of the femoral artery which was identified as the descending genicular artery for its peculiar course. On US axial scans the gescending genicular artery may be carefully distinguished from a large muscular branch to vastus medialis which arises more proximally from the lateral aspect of the femoral artery.
The progressive separation of the femoral vessels and the saphenous nerve suggested the proximity of the hiatal region but the origin of the descending genicular artery from the superficial femoral artery represented another and more precise landmark on US examination to identify the distal end (hiatal region) of the adductor canal (Figure 8).
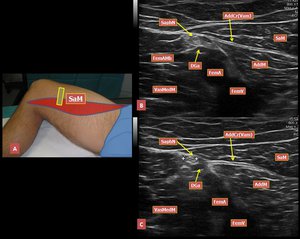
Fig.: Figure 8. A) Transducer orientation on the antero-medial aspect of the distal third of the thigh. B, C) Two adjacent axial US scans in the lower part of adductor canal where femoral vessels and saphenous nerve separate. The saphenous nerve is adjacent to the descending genicular artery which may not be confused with a large, more proximal, muscular branch of the femoral artery to vastus medialis. Legend: Sam, sartorius muscle; AddM, adductor magnus muscle; VasMedM, vastus medialis muscle; FemAMb, muscular branch of the femoral artery to the vastus medialis; FemA, femoral artery; FemV, femoral vein; DGa, descending genicular artery; AddCr(Vam), adductor canal roof (vastoadductor membrane); SaphN, saphenous nerve.
The origin of descending genicular artery from the superficial femoral artery was best assessed on coronal oblique US scans. The descending genicular artery gives immediately rise to its saphenous branch, which passes anteriorly to the adductor magnus rounded tendon, piercing the roof of the adductor canal, and moves inferiorly and medially toward the deep surface of sartorius muscle. The descending genicular artery (main trunk) was easily appreciable on axial and coronal oblique US scans, in particular coronal oblique US scans allowed the visualization of its course adjacent to the adductor magnus rounded tendon. It was impossible to demonstrate the saphenous nerve piercing the vastoadductor membrane accompanied by the saphenous branch of the descending genicular artery (Figure 9).
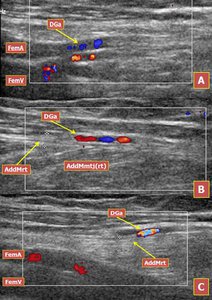
Fig.: Figure 9. A) Color-Doppler coronal oblique scan showing the origin of the descending genicular artery which emerges from the lateral aspect of the femoral artery wall. B) Color-Doppler coronal oblique US scan demonstrating the descending genicular artery moving downward to the knee joint anterior to the adductor magnus tendon and posterior to vastus medialis muscle. C) Color-Doppler coronal oblique US scan showing the relation between descending genicular artery and adductor magnus rounded tendon, which forms the medial wall of the adductor canal hiatus. Note the slight deflection of the femoral vessels passing through the adductor canal hiatus. Legend: DGa, descending genicular artery; AddMrt, adductor magnus rounded tendon; FemA, femoral artery; FemV, femoral vein; AddMmtj(rt), adductor magnus myotendinous junction (origin of the rounded tendon).
The subsartorial branch of the saphenous nerve was identified much more caudally, out of the Hunter’s canal, in the medial knee region for its close relation to the saphenous branch of the descending genicular artery, using this arterious vessel as an anatomical landmark, but this was beyond the scope of our study.
The US morphologic examination of the adductor canal hiatus was complex and some anatomical limits of this region were best assessed on coronal oblique scan planes. The medial margin of the hiatus is the adductor magnus tendon, which courses to the medial femoral condyle. The rounded tendon of adductor magnus was easily identified at its enthesis performing a coronal oblique scan, using the adductor tubercle of the medial femoral condyle as an osseous landmark. When the fibrillar echostructure of the adductor magnus tendon was correctly visualized without anisotropic artifact, a slight, progressive cranial motion of the transducer, always in the coronal oblique scan plane, allowed the visualization of the myotendinous junction of the tendon itself. The superficial femoral vessels were appreciable laterally to the myotendinous structure moving in a dorsolateral direction to become popliteal vessels. Adjacent coronal oblique scans, always using the rounded tendon of adductor magnus as a reference, aided the assessment of the region of “deflection” of the femoral vessels which corresponds to the adductor canal hiatus. In the hiatus, the femoral artery is anteromedial to the femoral vein (figure 10).
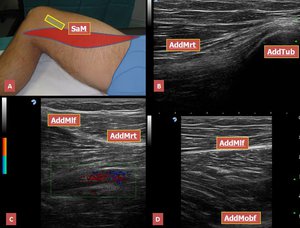
Fig.: Figure 10. A) Transducer orientation on the medial femoral condylar region. B) Coronal oblique US scan at the adductor tubercle of the medial femoral condyle; the adductor magnus rounded tendon shows the typical fibrillar pattern. C) Color-Doppler coronal oblique US scan at a more proximal level than A revealing the relations between adductor magnus rounded tendon and femoral vessels at the adductor canal hiatus. Femoral vessels may be seen passing through the adductor hiatus. D) Coronal oblique US scan at a level more proximal than B showing the oblique fibers of adductor magnus muscle which spread laterally to insert on the medial margin of the linea aspera and the longitudinal fibers which converge to form the rounded tendon. Legend: AddMrt, adductor magnus rounded tendon; AddTub, adductor tubercle; AddMlf, adductor magnus longitudinal fibers; AddMof, adductor magnus oblique fibers; SaM, sartorius muscle.

 Transducer orientation on the crural region at the apex of the femoral triangle. B) Axial MR section showing the vascular structures at the apex of the femoral triangle which is in continuity with the adductor canal. C) The deep fascia of sartorius muscle is in relation with the anterior aspect of the superficial femoral artery wall. D) Corresponding color-Doppler axial scan. Legend: SaM, sartorius muscle; SupFemA, superficial femoral artery; AddL, adductor longus muscle; RectF, rectus femoris muscle; VasMedM, vastus medialis muscle.")
 Transducer orientation on the anteromedial aspect of the thigh. B) Axial oblique US scan showing the neurovascular bundle inside the proximal third of the adductor canal. The saphenous nerve is lateral to the femoral artery; the femoral vein is posterior. The posterior wall is represented by adductor longus muscle. C) Corresponding color-Doppler axial scan showing the “honeycomb” echostructure of the saphenous nerve, adjacent to the arterial wall. Legend: SaM, sartorius muscle; SaphN, saphenous nerve; FemA, femoral artery; Fem V, femoral vein; VasMedM, vastus medialis muscle; AddL, adductor longus muscle.")
 Transducer orientation on the medial aspect of the middle third of the thigh. B, C) Two adjacent US axial scans demonstrating the perforating venous branch emerging from the medial aspect of the superficial femoral vein to move medially toward the great saphenous vein which is located in the superficial fascia, between sartorius (anterior) and gracilis muscles (posterior). At this level the posterior wall of the adductor canal is still formed by the adductor longus muscle. D) Corresponding axial MR section showing the great saphenous vein in the superficial fascia. Legend: SaM, sartorius muscle; FemA, femoral artery; FemV, femoral vein; VasMedM, vastus medialis muscle; AddL, adductor longus muscle; PerfBGSv, perforating branch of the great saphenous vein; GSv, great saphenous vein; GraM, gracilis muscle.")

 Schematic drawing illustrating the boundaries of the proximal and distal parts of the Hunter’s canal. Note that adductor canal hiatus is delimited medially by the longitudinal fibers of adductor magnus muscle and its rounded tendon, laterally by the oblique fibers of adductor magnus. C) Axial MR scan showing the hamstring part (longitudinal fibers) of the adductor magnus with its myotendinous junction and the adductor part (oblique fibers) which inserts via an aponeurosis on the medial margin of the linea aspera. Legend: SaM, sartorius muscle; FemA, femoral artery; FemV, femoral vein; VasMedM, vastus medialis muscle; AddMmtj(rt), adductor magnus myotendinous junction (origin of the rounded tendon); AddMobf, oblique fibers of adductor magnus; MedMla, medial margin of linea aspera; SemimM, semimembranosus muscle; SemitM, semitendinosus muscle; GraM, gracilis muscle.")
, adductor magnus myotendinous junction (origin of the rounded tendon); GraM, gracilis muscle; GSaphV, great saphenous vein; AddTub, adductor tubercle.")

 Transducer orientation on the antero-medial aspect of the distal third of the thigh. B, C) Two adjacent axial US scans in the lower part of adductor canal where femoral vessels and saphenous nerve separate. The saphenous nerve is adjacent to the descending genicular artery which may not be confused with a large, more proximal, muscular branch of the femoral artery to vastus medialis. Legend: Sam, sartorius muscle; AddM, adductor magnus muscle; VasMedM, vastus medialis muscle; FemAMb, muscular branch of the femoral artery to the vastus medialis; FemA, femoral artery; FemV, femoral vein; DGa, descending genicular artery; AddCr(Vam), adductor canal roof (vastoadductor membrane); SaphN, saphenous nerve.")
 Color-Doppler coronal oblique scan showing the origin of the descending genicular artery which emerges from the lateral aspect of the femoral artery wall. B) Color-Doppler coronal oblique US scan demonstrating the descending genicular artery moving downward to the knee joint anterior to the adductor magnus tendon and posterior to vastus medialis muscle. C) Color-Doppler coronal oblique US scan showing the relation between descending genicular artery and adductor magnus rounded tendon, which forms the medial wall of the adductor canal hiatus. Note the slight deflection of the femoral vessels passing through the adductor canal hiatus. Legend: DGa, descending genicular artery; AddMrt, adductor magnus rounded tendon; FemA, femoral artery; FemV, femoral vein; AddMmtj(rt), adductor magnus myotendinous junction (origin of the rounded tendon).")
 Transducer orientation on the medial femoral condylar region. B) Coronal oblique US scan at the adductor tubercle of the medial femoral condyle; the adductor magnus rounded tendon shows the typical fibrillar pattern. C) Color-Doppler coronal oblique US scan at a more proximal level than A revealing the relations between adductor magnus rounded tendon and femoral vessels at the adductor canal hiatus. Femoral vessels may be seen passing through the adductor hiatus. D) Coronal oblique US scan at a level more proximal than B showing the oblique fibers of adductor magnus muscle which spread laterally to insert on the medial margin of the linea aspera and the longitudinal fibers which converge to form the rounded tendon. Legend: AddMrt, adductor magnus rounded tendon; AddTub, adductor tubercle; AddMlf, adductor magnus longitudinal fibers; AddMof, adductor magnus oblique fibers; SaM, sartorius muscle.")