ECR 2010 / C-2713
Radiology of hypothalamic lesions: A pictorial essay depicting characteristic hypothalamic pathologies
Congress:
ECR 2010
Poster Number:
C-2713
Type:
Scientific Exhibit
Keywords:
Neuroradiology brain, Neuroradiology peripheral nerve, Neuroradiology spine
Authors:
A. J. B. Baxi, M. belman, T. Nagendra, S. Vidyasagar, K. L. Tourani; Hyderabad/IN
DOI:
10.1594/ecr2010/C-2713

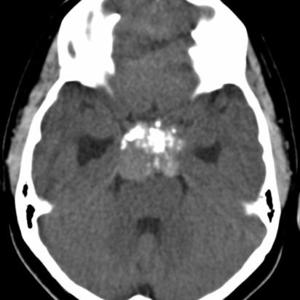
Fig. 1:
Partially calcified sella mass- craniopharyngioma

Fig. 2:
Craniopharangioma with cyst and calcification

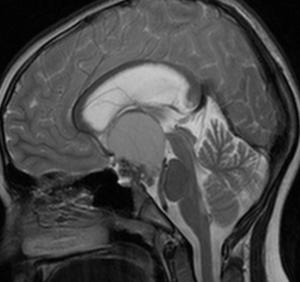
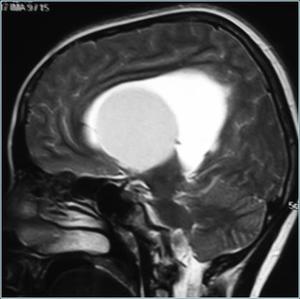
Fig. 3:
Craniopharangioma- Sag T2

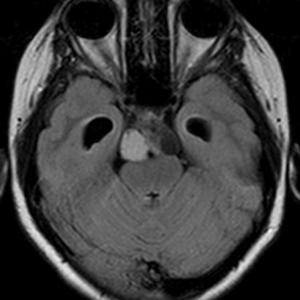
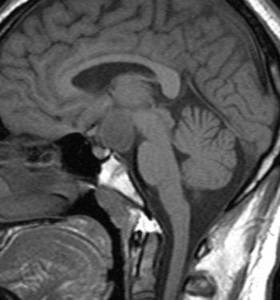
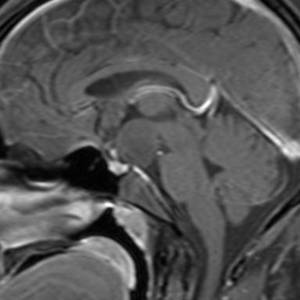
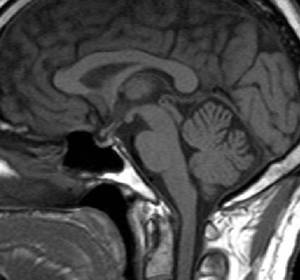
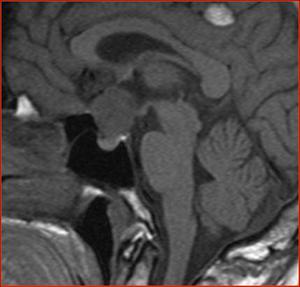
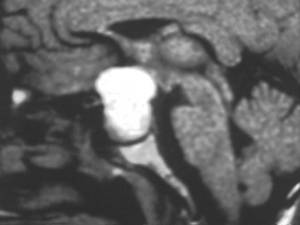
Fig. 4:
Saggital T1-Hypothalamic Hamartoma

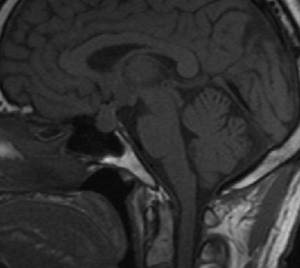
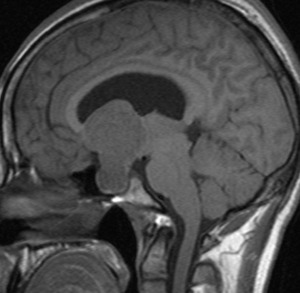
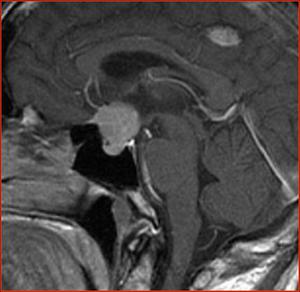
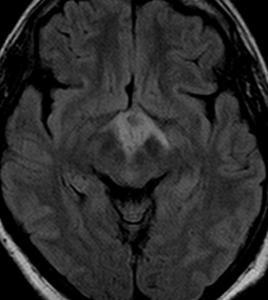
Fig. 5:
Non enhancing Hypothalamic hamartoma

Fig. 6:
Fig6-Bilateral opticochiasmatic hypothalamic glioma

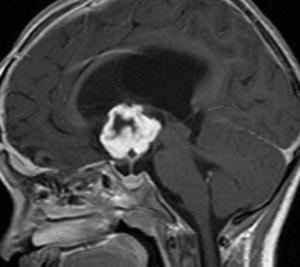
Fig. 7:
Enhancing hypothalamic glioma.

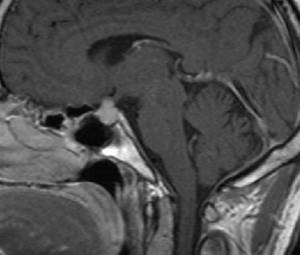
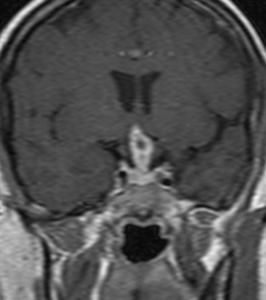
Fig. 8:
Ti sagittal-Diffuse enlargement of pituitary ,infundibulum and hypothalamus.

Fig. 9:
CE sagittal T1- lymphocytic hypophysitis.symmetric enlargement of the pituitary...

Fig. 10:
Lymphocytic hypophysitis-complete shrinkage of mass after high glucocorticoid...

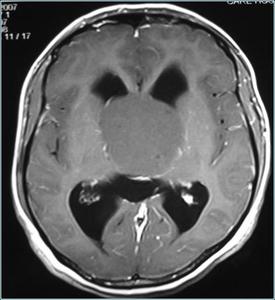
Fig. 11:
Pituitary macroadenoma with suprasellar extension

Fig. 12:
Enhancing pituitary macroadenoma with suprasellar extension.

Fig. 13:
T1 isointense Meningioma

Fig. 14:
Enhancing meningioma with dural tail sign

Fig. 15:
TB granuloma involving hypothalamus,optic chiasma and optic tract

Fig. 16:
TB granuloma involving hypothalamus ,optic chiasma and optic tract.

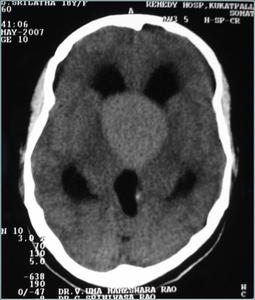
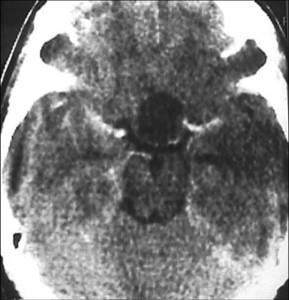
Fig. 17:
Hyperdense colloid cyst on CT

Fig. 18:
Colloid cyst on sagittal T2

Fig. 19:
Post contrast T1 image showing non-enhancing colloid cyst

Fig. 20:
Dermoid cyst with fatty attenuation on CT

Fig. 21:
Sag T1 image showing hyperintense dermoid cyst

Fig. 22:
Rathke cleft cyst.

Fig. 23:
Radiation necrosis of optic chiasma following radiotherapy for pituitary adenoma

Fig. 24:
Radiation necrosis of optic chiasma following radiotherapy for pituitary...

Fig. 25:
Hypothalamic encephilitis.

Fig. 26:
Hypothalamic encephilitis.

Fig. 27:
Hypothalamic encephilitis.

Fig. 28:
Aspergillous granuloma.Plain CT shows hyperdense lesion in sellar region...

Fig. 29:
Aspergillous granuloma extending into middle and posterior cranial fossa

Fig. 30:
Aspergillous granuloma secondary to sinusitis and mastoiditis.

Fig. 31:
Hypothalamic glioma

Fig. 32:
Craniopharyngioma showing peripheral enhancement.

Fig. 33:
Pituitary macroadenoma with hemorrhage.