The Atypical imaging presentation of CNS tuberculosis includes:
- Gaint tuberculomas mimicking the high grade glioma
- Pitutary tuberculoma
- Inflammatory endarteritis obliterens due to involvment of arteries which course through exudates causing spasm and intimal changes resulting in thrombosis and infarction. Infarctions are more common in children and most commonly involve perforating branches supplying the basal ganglia.
- Arteritis causing Moya Moya pattern
- Extraaxial tuberculoma mimicking meningioma
Although both CT and MRI can demonstrate these findings but MRI detects it much earlier. Similarly, in atypical imaging presentation advance MR imaging such as diffusion imaging, and proton magnetic resonance spectroscopy techniques are important for better tissue characterization as described above.
Giant tuberculoma:
The Atypical imaging presentation of CNS tuberculosis includes:
· Gaint tuberculomas mimicking the high grade glioma
· Pitutary tuberculoma
· Inflammatory endarteritis obliterens due to involvment of arteries which course through exudates causing spasm and intimal changes resulting in thrombosis and infarction. Infarctions are more common in children and most commonly involve perforating branches supplying the basal ganglia.
· Arteritis causing Moya Moya pattern
· Extraaxial tuberculoma mimicking meningioma
Although both CT and MRI can demonstrate these findings but MRI detects it much earlier. Similarly, in atypical imaging presentation advance MR imaging such as diffusion imaging, and proton magnetic resonance spectroscopy techniques are important for better tissue characterization as described above.
Giant Tuberculoma
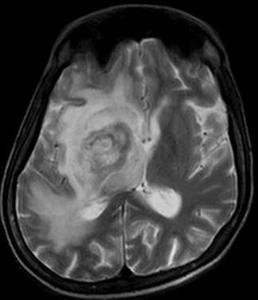
Fig.: Fig.: T2W axial image showing hypointense lesion in right basal ganglia region with surrounding hyperintense edema
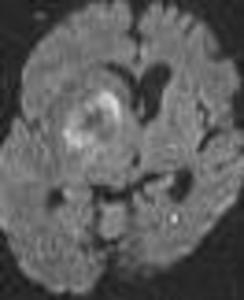
Fig.: Fig.: Diffusion image showing restricted diffusion in periphery of lesion

Fig.: Fig.:ADC image showing corresponding dark signal
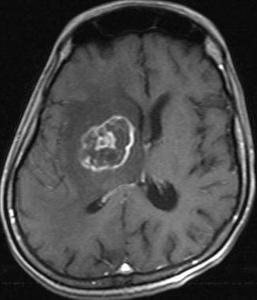
Fig.: Fig.:Post contrast image showing peripheral ring enhancement with enhancing intra lesion area mimicking high grade glioma.
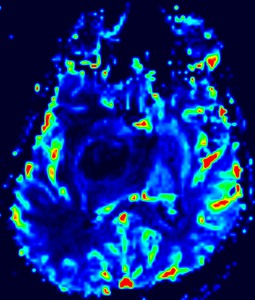
Fig.: Fig.:Perfusion image showing totally hypoperfused lesion which favors benign lesion
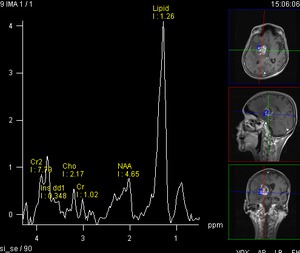
Fig.: Fig.:Multivoxel Proton MR spectroscopy image showing a high lipid peak favors tuberculoma
GBM(Glioblastoma Multiforme
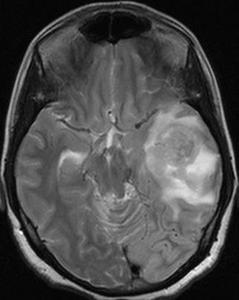
Fig.: Fig.: T2W image showing hypo to isointense lesion in left temporal lobe
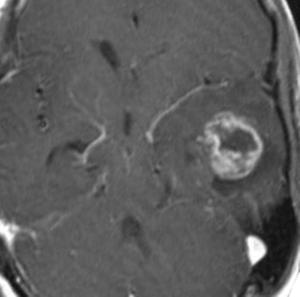
Fig.: Fig.: Contrast image showing heterogenous enhancement of lesion
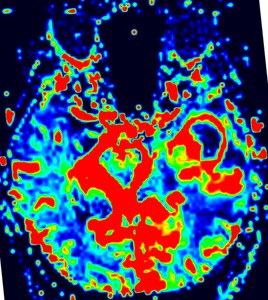
Fig.: Fig.:Perfusion image showing hyper perfusion of periphery and solid part of lesion which favor aggressive lesion
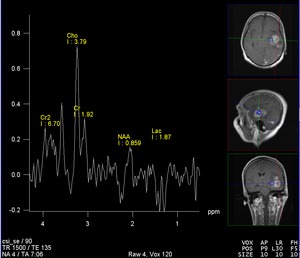
Fig.: Fig.: Multivoxel Proton MR spectroscopy image showing large Choline with reduced NAA peak conforming high grade glioma
Pituitary Tuberculoma-
This patient presented with SIADH and on imaging ring enhancing lesion was detected in sellar and supra sellar region. Single voxel proton MR spectroscopy using 135 TE was performed which revealed large lipid lactate peak with reduced NAA and no change in choline peak as compare to voxel placed in normal parenchyma.
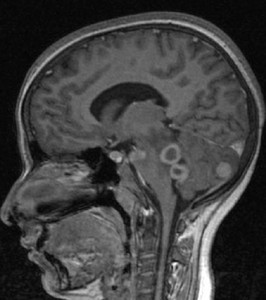
Fig.: Postcontrast T1 image shows a ring enhancing lesion in anterior pituitary along with intraventricular and cerebellar tuberculomas
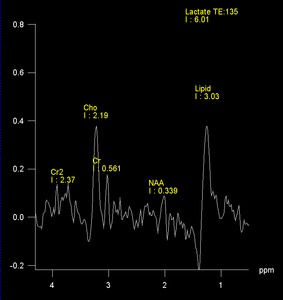
Fig.: Fig.: Single voxel proton MR spectroscopy using 135 TE, showing large lipid lactate peak with reduced NAA and no change in choline peak as compare to voxel placed in normal parenchyma
Vasculitis and various presentations
1. Enhnancing exhudates along MCA causing its inflammation, occlusion and large parenchymal infarct.
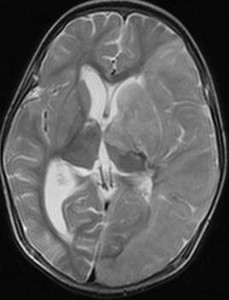
Fig.: Fig.: T2W image showing hyperintense large left MCA region infarct
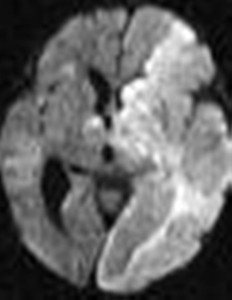
Fig.: Fig.: Diffusion Weighted image showing restricted diffusion
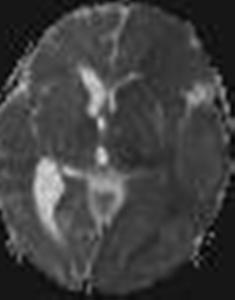
Fig.: Fig.: ADC image showing corresponding dark ADC signal

Fig.: Fig.: TOF( Time of flight ) angiogram reconstructed image showing complete occlusion of left ICA and MCA
2. Exudates along basal cistern can cause vasculitis of perforating branches and resultant bilateral basal ganglia infarct.
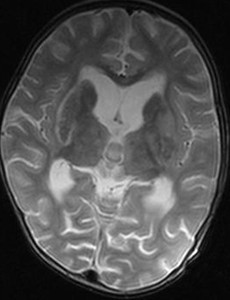
Fig.: Fig.: T2W image showing hypointensity in bilateral basal ganglia region. There is hyperintense rim surrounding right putamen
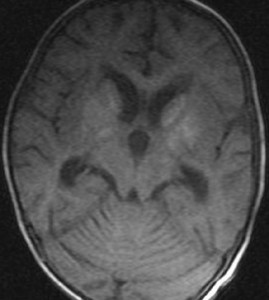
Fig.: Fig.: T1W image showing mild bilateral basal ganglia hyperintensity
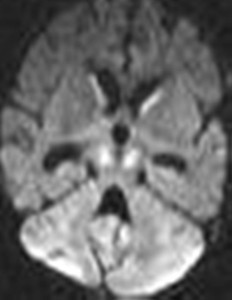
Fig.: Fig.: Diffusion image showing restricted diffusion in bilateral caudate nucleus and cerebral peduncles.
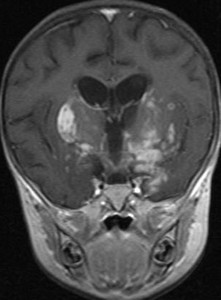
Fig.: Fig.: Post contrast T1W showing enhancing exudates along basal cisterns and both MCA with enhancement of right putamen. Also note ring enhancing lesion in left basal ganglia region
3. Cortical laminar necrosis: tuberculous vasculitis causing small peripheral vessel occlusion, ischemia which can later presenting as cortical laminar necrosis( usually after 3-4 wks) . cortical laminar necrosis appears as hyperintensity on T1W image and shows enhancement on post contrast image.
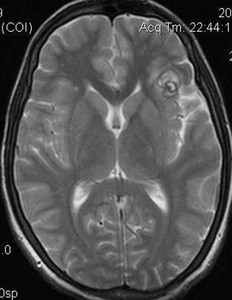
Fig.: Fig.: T2 W image showing hyperintense lesion in left Sylvain fissure with hypointense rim. Another T2 hypointense foci seen with in the lesion
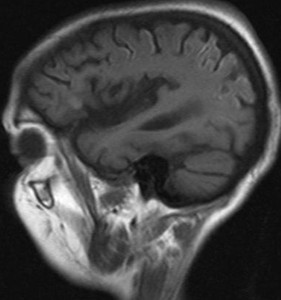
Fig.: Fig.: T1W image showing hyper intensity along left posterior parietal convexity along the gyri. Also, note that the left Sylvain fissure lesion hyperintensity
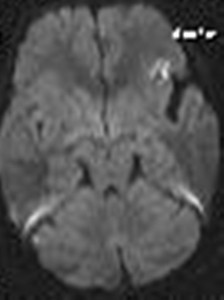
Fig.: Fig.: Diffusion image showing restricted diffusion in the lesion
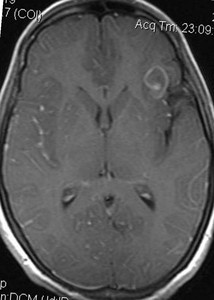
Fig.: Fig.: Post contrast image showing regular rim enhancement of lesion
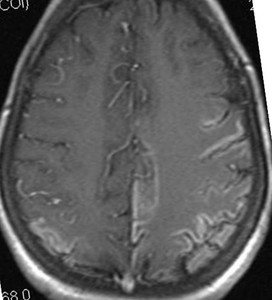
Fig.: Fig.: Post contrast image showing increased enhancement along left posterior parietal cortex in gyral pattern
4. Sometimes CNS vasculitis along with other typical findings, can present with parenchymal hemorrhage.
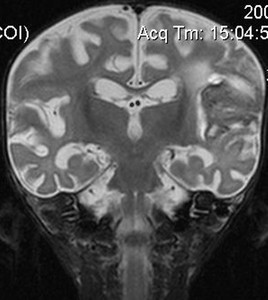
Fig.: Fig.: T2W coronal image showing mixed intensity and predominantly hypointense lesion along left sylvian cistern and adjacent parenchyma
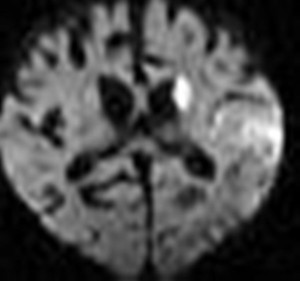
Fig.: Fig.: Diffusion image showing restricted diffusion along left caudate nucleus and left parietal parenchyma
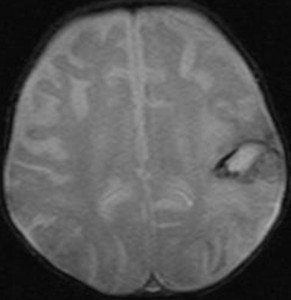
Fig.: Fig.: Gradient image showing hypointense rim along the left parietal hyperintense lesion suggestive of resolving hemorrhage
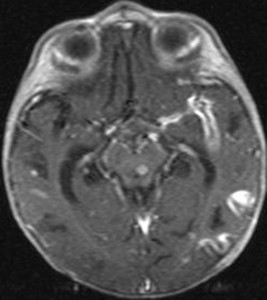
Fig.: Fig.: Post contrast axial image showing enhancing exudates along left MCA
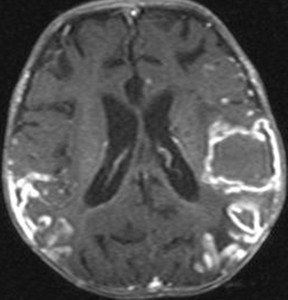
Fig.: Fig.: Post contrast image showing enhancing plaque like exudates in bilateral parietal convexities and rim enhancement of left parietal lobe lesion
5. CNS vasculitis can rarely cause bilateral ICA and proximal MCA narrowing presenting as moya moya pattern.
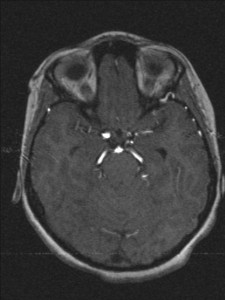
Fig.: Fig.: Time of flight MR angiogram image shows narrowing of distal ICAs proximal MCAs with collateral formation
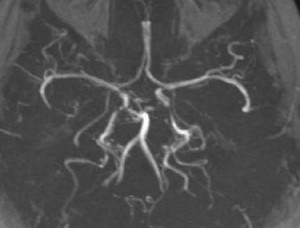
Fig.: Fig.: Time of flight MR angiogram image in another patient with Moya Moya pattern
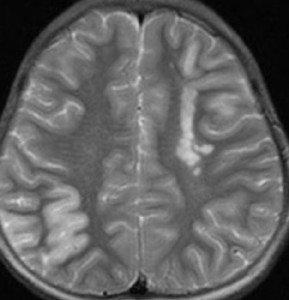
Fig.: Fig T2W image showing acute infarcts in the distal MCA territory on the both sides. Chronic infarcts are seen in left centrum semiovale
Extraaxial tuberculoma along conxexities can mimic meningioma on conventional MR imaging however, MR spectroscopy helps to differentiate by showing a large lipid/lactate peak.
The typical pattern of enchantment seen in CNS tuberculosis is rim enhancement . There are various other lesions which also show rim enhancement on post contrast image. Differentials of ring enhancing lesion other than granuloma include:
- Abscess
- GBM
- Cystic metastasis
- Lymphoma
- Demyelination
- Infarct
- Resolving hematoma
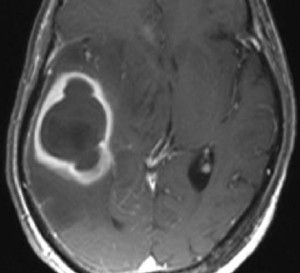
Fig.: Fig.: Postcontrast T1 axial image in a case of cerebral abscess
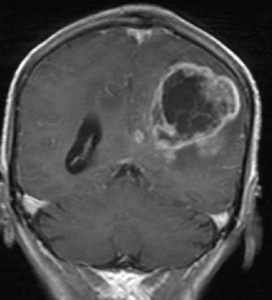
Fig.: Fig.: Postcontrast T1 coronal image in a case of GBM
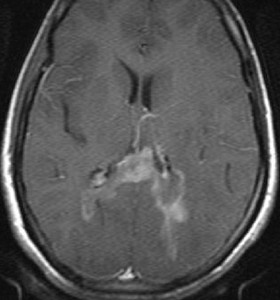
Fig.: Fig.: Postcontrast T1 Axial image in a case of Lymphoma
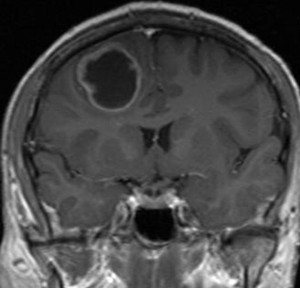
Fig.: Fig.: Postcontrast T1 coronal image in a case of Metastasis
