All cases were confirmed at histology as ductal adenocarcinoma of the pancreas.
Resection margin with microinfiltration (R+) was present in 11 cases (18,5%) of whom 9 localized at the SMA margin and 2 at the pancreatic resection margin.
In 37 patients the lesion was located in the pancreas head/uncinate process and in 8 patient in the pancreatic body,
with a lesion dimension ranging between 15mm and 60mm.
CT examination considered 67 vessels (42 veins and 25 artery) as infiltrated and 43 vessels (12 veins and 31 artery) as not infiltrated,
with an overall judgement of venous infiltration in 24 patients,
arterial in 5 patients and artero-venous in 18 patients.
In 7 cases the tumor was classified at CT as not locally advanced,
because of the absence of signs of vascular infiltration.
Regarding the lenght of vascular encasement,
in 38 cases it was >20mm and in 9 cases it was <20mm.
Sixtyfour vessels were resected (52 venous tract,
12 artery-5 SMA and 7 celiac trunk).
Pathological analysis demonstrated the presence of infiltration in 46 out of 64 resected vessel (72%).
Regarding the 67 vessels considered as infiltrated at CT,
pathology confirmed the presence of infiltration in 50 vessels (12 artery and 38 veins).
Four artery and 38 veins were effectively resected,
while 8 non resected SMA were considered infiltrated only indirectly,
because histology showed a R+ on the SMA margin.
False positive vessels were 17 (4 veins and 13 artery) of whom 11 had been resected,
while in the remaining 6 non resected artery,
the absence of infiltration was obtained at intraoperative examination of the perivascular fat tissue (1 case) or indirectly because of an negative (R0) SMA resection margin (5 cases).
Eleven vessels (1 artery and 10 veins),
considered as not infiltrated at CT,
were otherwise resected: histology confirmed the absence of infiltration in 7 vessels (1 artery e 6 vein),
while 4 veins resulted to be infiltrated.
In the evaluation of vascular infiltration,
CT showed overall sensitivity of 93% (in particular,
100% for venous and 90% for arterial infiltration),
specificity of 70% (71% for venous and 67% for arterial infiltration) and diagnostic accuracy of 81% (77% for venous and 85% for arterial infiltration),
positive predictive value 75% (48% for venous and 90% for arterial infiltration),
negative predictive value 91% (100% for venous and 67% for arterial infiltration) (Fig 1).
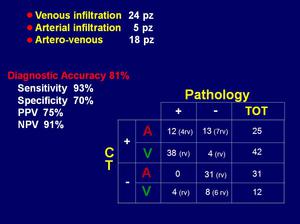
Fig.: Results: vascular infiltration
At CT,
the suspicion of retroperitoneal fat corresponding to the SMA margin infiltration was posed in 31/54 cases,
judging 22 cases as macroinfiltrated and 9 cases as microinfiltrated.
Histology demonstrated the presence of infiltration of the fat tissue (T3) in 29 cases,
in particular in 27 out of 31 case (87%) suspected at MDCT; more in detail,
infiltration was confirmed in 21/22 (95%) cases judged as macroinfiltrated at CT and in 6/9 (76%) microinfiltrated cases.
Infiltration of the mesenteric/mesocolic root was suspected at CT in 23 cases and was confirmed by histology in 20 cases (the false positive CT diagnoses were due to chronic inflammation of the fat tissue).
Overall,
in the evaluation of the peripancreatic fat tissue infiltration,
CT showed a sensitivity and a specificity of 96% and 91% respectively and a diagnostic accuracy of 91%.
The positive and negative predictive values resulted to be 85% and 97%,
respectively.
(Fig.2)
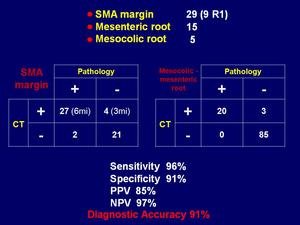
Fig.: Results: SMA margin and mesenteric/mesocolic root infiltration
At CT,
7 patients resulted to be resectable,
23 borderline resectable and 24 palliative resectable and at pathology 7,
30 and 17 respectively,
with concordance in 39/54 cases (72%).
In judging resectability CT showed sensibility of 85%,
specificity of 60%,
PPV of 68% NPV of 80% and diagnostic accuracy of 72%.
The corresponding dates in judging unresectability was 94%,
78%,
67%,
97% e 83% (Fig.
3).
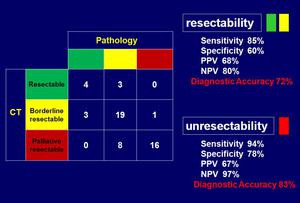
Fig.: Results: resectability judgement
Regarding statistical analysis,
6 patients (11%) were excluded,
because they died in the perioperative period because of complication.
Of the remaining 48 patients,
16 were still alive at the moment of the study (with a follow-up ranging between 5 and 113 months) and 32 were died (with a follow-up between 1 and 100 months).
Survival was 84% and 57% at 6 month and 1 year respectively,
and particularly 1 year survival was 100% for patients identified as resectable,
75% for borderline resectable and 28% for palliative resectable.
No statistical correlation with survival existed by considering location of the tumor (p=0,5),
size of the tumor at CT (p=0,16) and length of tumor-vessel contact (p=0,75).
A statistically significant correlation with survival was obtained by considering type of vessel infiltrated (p=0,03),
retroperitoneal fat corresponding to the SMA margin (p=0,03),
mesenteric/mesocolic root(p=0,02) and histological SMA margin (p=0,03) infiltration.
Finally judgement of resectability at MDCT resulted to be strongly related to survival (p=0,0008) (Fig.
4).
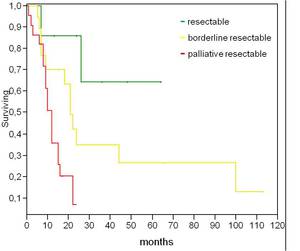
Fig.: Kaplan-Meier survival curves, up to 113 months, based on the judgement of resectability at MDCT (p=0,0008)




")