We included 54 patients with locally-advanced pancreatic adenocarcinoma submitted to surgery with vascular resection.
All the exams were performed by a multidetector CT (Light Speed Plus,
GE Medical System,
Milwaukee USA or Light Speed VCT,
GE Medical System,
Milwaukee USA); the study was done after gastroduodenal hyperdistension,
obtained by oral administration of 750/1000 mL of water and by pharmacological hypotonization (Buscopan® o GlucaGen®),
in order to improve the visualization of the relationships between the gastric wall and pancreatic body and between the duodenal wall and the pancreatic head.
All the CT studies were performed before and after intravenous administration of high concentrated iodinated contrast medium (Iomeron® 400),
at 4mL/s injection flow-rate.
Post-contrast scans were performed both in pancreatic (35”delay; slice thickness 2.5-1,25 mm,
reconstruction interval 1.25-0,6 mm ) and venous phases (70” delay; slice thickness 1.25-0,6 mm,
reconstruction interval 0.6 mm).
All native images were sent to a dedicated workstation (Advantage Windows 4.0,
GE Medical System,
Milwaukee USA) and processed with multiplanar reconstruction (MPR) in order to evaluate in different planes the relationship between the neoplastic lesions and the surrounding structures.
At CT we evaluated the following criteria: vascular involvement (celiac trunk arteries,
superior mesenteric artery,
portal-mesenteric venous axis),
fat tissue infiltration (mesenteric root and transverse mesocolon,
retroperitoneal fat corresponding to the SMA margin).
For the evaluation of the vascular involvement,
we used the following grading system published by Mazzeo et al.
(2007) [4]: no contact between neoplasm and vessel (grade 0); focal contiguity between neoplasm and vessel,
without modifications of the vessel caliber (grade I); the neoplasm surrounds partially or completely the vessel,
without caliber reduction (grade II); the neoplasm surrounds partially or completely the vessel,
with reduction or obstruction of the vessel lumen (grade III).
On the basis of the results of this work,
we considered as infiltrated vessels with grade II and III (positive predictive values - PPV - of infiltration 80%) and not infiltrated vessels with grade 0 and I (negative predictive value – NPV - of infiltration 82%) [4].
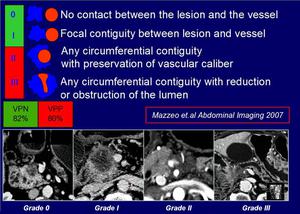
Fig.: Vascular infiltration grading system
Regarding neoplastic infiltration of fat tissue,
it was suspected in the presence of one of the following signs (Fig.
2):
- tissue obliteration,
representing a sign of macro-infiltration,
according to a study published by Mazzeo at al.
in 2010,
with a PPV of 94%;
- alteration of the tissue density,
classified as suspicion of micro-infiltration with a PPV of 50% [5];
In all patient was evaluated the presence of infiltration at the level of mesenteric and transverse mesocolic root and the fat tissue corresponding to SMA margin identifiable as the fat tissue between the left margin of the head/uncinate process and the right wall of the proximal 3–4 cm of the superior mesenteric artery.
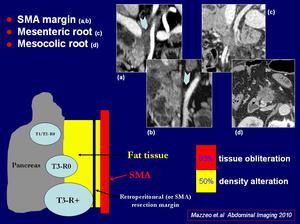
Fig.: Imaging findings of fat tissue infiltration
On the basis of both vascular and fat tissue involvement,
patients were divided into 3 different groups: resectable (absence of vascular and fat tissue infiltration),
borderline resectable (peripancreatic and venous infiltration liable to resection,
likely R0) and palliative resectable (arterial or venous infiltration associated to peripancreatic infiltration,
liable to resection likely R+).
All CT local staging findings and the overall resectability judgement were compared to histopathological results after resection.
In order to identify possible prognostic factors of survival,
Kaplan-Meier survival curves were obtained by considering size and location of the tumor,
length of tumor-vessel contact (cut-off 20mm),
type of vessel infiltrated (venous,
arterial,
artero-venous),
retroperitoneal fat tissue and mesenteric/mesocolic root infiltration,
judgement of resectability at MDCT and histological SMA margin infiltration.


