Imaging Techniques
Magnetic resonance imaging (MRI) is the most reliable imaging technique to define the depth of myometrial invasion and the degree of cervical involvement pre-operatively.
Transvaginal ultrasound (TVUS) is used for initial assessment of the endometrium in patients who present with abnormal uterine bleeding,
however MRI has been found to be more accurate then TVUS in assessment of myometrial invasion (12).
CT can be used to differentiate stage I and II (disease limited to the uterus) from stage III and IV (extra-uterine spread of disease) in endometrial carcinoma.
However several studies have demonstrated the accuracy for the detection of deep myometrial invasion and cervical involvement to be far inferior than that of MRI (13,14).
MRI staging acts as an important triage to place patients in correct treatment arms.
These may be surgical and non-surgical,
may involve radiotherapy,
and may involve treatment at a specialist gynaecological oncology institution (12).
Staging tries to reduce variation in treatment across centres.
As the initial provisional staging is radiological,
based on MR imaging,
attempts have been made to standardise MR techniques.
The following are the current ESUR guidelines for MRI cancer staging protocols published in 2009 (13).
ESUR protocol
- Fasting 3-6 hours.
- Antiperistaltic agent,
e.g.
buscopan,
to reduce artefact from bowel movement (unless contra-indicated).
- Empty bladder prior to examination to reduce artefact.
- High resolution T2 weighted imaging of the pelvis in sagittal,
axial oblique (perpendicular) and coronal oblique (parallel) to the uterine cavity (Figure 1). If there is suspected cervical involvement,
axial oblique imaging perpendicular to the long axis of the endocervical channel is recommended.
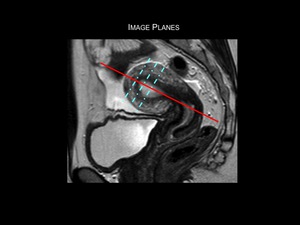
Fig.: Figure 1: Image planes for high-resolution T2-weighted imaging of the uterus. Initial high resolution T2-weighted sagittal images of the pelvis are obtained. Axial oblique images are obtained by scanning perpendicular (dotted blue lines) to the long axis of the endometrial cavity (solid red line). These sequences can then be used for accurate assessment of myometrial invasion by tumour. If there is suspected cervical invasion, further imaging is recommended on a plane perpendicular to the long axis of the endocervical canal.
- For assessment of para-aortic lymph node enlargement,
metastases and complications e.g.
hydronephrosis,
extended FOV imaging is required.
- For the diagnosis of deep myometrial invasion as well as for use in atrophic uteri,
associated adenomyosis and fibroids,
and for suspected Stage IV endometrial carcinoma,
contrast-enhanced imaging is suggested for higher accuracy.
2D or 3D techniques may also be performed with optimal tumour contrast timing to be between 90 and 150s (10).
Normal uterine anatomy on MRI
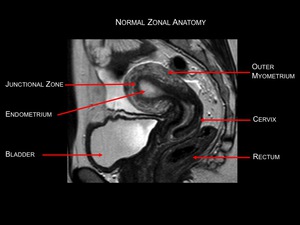
Fig.: Figure 2: Normal zonal anatomy in a pre-menopausal female. High resolution sagittal T2-weighted image. The endometrium demonstrates
high signal intensity. The junctional zone or inner myometrium is demonstratesd by a band of low signal intensity. The intermediate signal outer layer represents the remainder of the myometrium. Zonal anatomy in post-menopausal women is less clear.
Tumour Appearance
On T2-weighted imaging,
endometrial carcinoma is of lower signal intensity than the endometrium.
On T1-weighted post-contrast imaging the tumours are of lower signal intensity than the enhancing myometrial tissue. On dynamic imaging,
the tumour is seen to enhance slower than the adjacent myometrium.
Non-contrast T1-weighted imaging is of no benefit in the evaluation of endometrial carcinoma since the endometrium,
myometrium and carcinoma all demonstrate similar intermediate signal intensities,
therefore differentiation is not possible (9,14).
Stage I: Tumour confined to the uterine body
The survival differences between stage IA and IB in the previous FIGO staging system were minimal so these two substages have now been combined as stage IA.
The previous Stage IC is now classified as stage IB.
On T1-weighted post-contrast imaging the tumour demonstrates poor enhancement and can be identified within the avidly enhancing myometrium. T2-weighted sagital and axial oblique imaging can be used to determine the degree of myometrial invasion.
Stage IA: No or less than one-half of myometrial invasion (Figures 3 & 4).
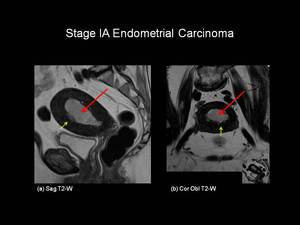
Fig.: Fig 3: Stage IA Endometrial carcinoma. Sagittal T2-weighted (a) and axial oblique T2-weighted (b) images in a post-menopausal female. On the T2-weighted images the endometrial cavity is distended with intermedaite signal intensity tumour (red arrows). The tumour has invaded the anterior myometrium by less than 50% (yellow arrows).
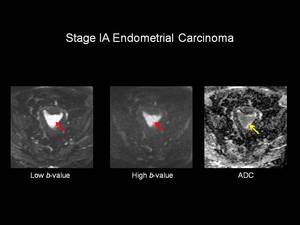
Fig.: Figure 4: Stage IA Endometrial Carcinoma. Axial Diffusion Weighted Imaging (DW-MRI). Imaging has been obtained from the same patient used in Figure 3. The uterine cavity is distended with high signal intensity material on the low b-value series which remains of high signal intensity on the high b-value series (red arrows). On the corresponding Apparent Diffusion Coefficient (ADC) map the lesion is of low signal intensity (yellow arrow) in keeping with tumour. This was histologically confirmed to represent grade 2 endometrial adenocarcinoma.
Stage IB: Invasion equal to or more than one half of the myometrium (Figures 5 & 6).
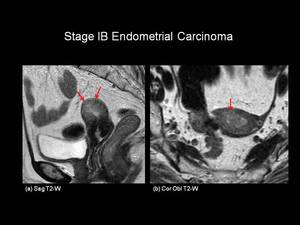
Fig.: Figure 5: Stage IB Endometrial Carcinoma. Sagittal (a) and coronal oblique (b) T2-weighted images in a post-menopausal female. Intermediate signal intensity tumour is seen distending the endometrial cavity with loss of the normal low signal intensity junctional zone. The tumour is seen to extend through greater than 50% of the myometrium (red arrows), but does not breach the uterine serosa.

Fig.: Figure 6: Endometrial Carcinoma. Sagittal T2-weighted (a) and sagittal T1-weighted fat suppressed post-gadolinium (b) images in a post menopausal female. On the T2-weighted image, the endometrium is distended with intermediate signal intensity of tumour (red arrow). There is suspicion of deep myometrial involvement, however the post-contrast images demonstrate that there is actually less than 50% myometrial invasion (yellow arrows) making this Stage IA endometrial carcinoma. Confirmed histopathologically following hysterectomy.
Limitations and Pitfalls in the Assessment of Myomometrial Invasion (16)
There are several factors that can limit accurate assessment of myometrial invasion,
these include:
1. Benign uterine disease
Leiomyomas (Figure 7) and adenomyosis (Figure 8) can mimic deep endometrial invasion and therefore be responsible for overstaging of myometrial invasion.
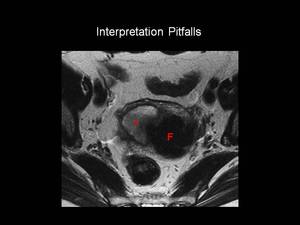
Fig.: Figure 7: Axial oblique T2-weighted image in a post-menopausal female. A large left-sided uterine fibroid (F) demonstrates low signal intensity on T2-weighted imaging and can be seen to distort the normal zonal anatomy of the uterus. It is difficult to assess the degree of myometrial invasion by the intermediate signal intensity of the tumour (T).
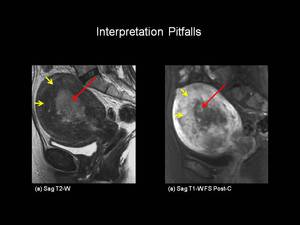
Fig.: Figure 8: Stage 1A Endometrial carcinoma. Sagittal (a) T2-weighted and T1-weighted (b) fat suppressed post- gadolinium images in a post menopausal female. There is intermediate signal intensity tumour seen distending the endometrial cavity (red arrows). The juntional zone is widened with evidence of adenomyosis (yellow arrows) making evalution of myometrial invasion difficult. This tumour was Stage IA on histopathology.
2. Polypoid tumours
Polypoid tumours within the uterine cavity may result in myometrial thinning,
which may result in understaging of endometrial carcinoma (Figure 9).
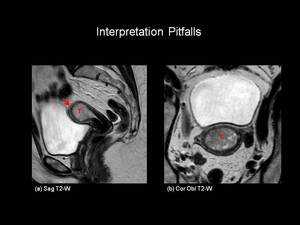
Fig.: Figure 9: Stage IA Endometrial carcinoma. Sagittal (a) and coronal-oblique (b) T2-weighted images in a post-menopausal female. There is a large intermediate signal intensity tumour (T) expanding the endometrial cavity. The tumour disrupts the normal low signal intensity of the junctional zone at the uterine fundus (red arrow) but does not involve greater than 50% of the myomterum indicating Stage IA disease. Myometrial thinning makes assessment of depth of invasion difficult.
3.
Tumours of the uterine cornu
These are difficult to assess since the myometrium in this region is thin,
and this may adversely affect staging of endometrial carcinoma within this area.
4.
Atrophy of the juntional zone
This may result in understaging of endometrial carcinoma.
Dynamic contrast enhanced magnetic resonance imaging (DCE-MRI; Figures 6,
8,
10,
11) and diffusion weighted MRI (DW-MRI; Figure 6) can be included in imaging protocols for staging patients with endometrial carcinoma. These techniques enable more accurate assessment of the depth of myometrial invasion especially in the presence of the pitfalls mentioned above. It has been shown that the combination of DCE-MRI and T2W imaging offers the highest efficacy for staging patients with endometrial carcinoma. In one study the depth of myometrial invasion was correctly determined in 78% of cases on T2 weighted-imaging,
increasing to 92% with the addition of DCE-MRI (15).
Stage II: Tumour invades cervical stroma,
but does not extend beyond the uterus
On T2-weighted imaging the tumour is of intermediate signal against a background of low signal intensity normal cervical stroma (Figure 10).
Post-contrast T1-weighted imaging is also used to improve accuracy and can help to differentiate true cervical invasion from endometrial polyps within the endocervical channel (17).
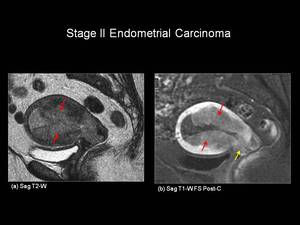
Fig.: Figure 10: Stage II Endometrial Carcinoma. Sagittal T2-weighted (a) and sagittal T1-weighted post gadolinium (b) in a post-menopausal female. There is intermediate T2-W signal intensity tumour filling and expanding the endometrial cavity (red arrows). In addition the tumour is seen to extend into the anterior lip of the cervix (yellow arrow). Note: tumour is seen to enhance less than the avidly enhancing myometrium.
Stage III: Local and/or regional spread of the tumour
Stage IIIA: Tumour invades the serosa of the corpus uteri and/or adnexae (Figure 11).
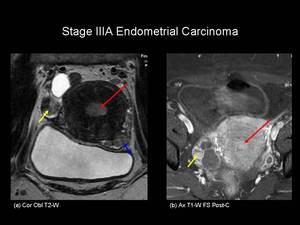
Fig.: Figure 11. Stage IIIA Endometrial carcinoma. Coronal oblique T2-weighted (a) and axial post-contrast T1-weighted fat saturated images through the pelvis in a postmenopausal female. The endometrial cavity is expanded by intermediate T2-W signal intensity material which shows enhancement following gadolinium administration (red arrows). In addition there is an enhancing metastatic nodule seen on the right ovary (yellow arrows) and a peritoneal deposit seen posterior to the urinary bladder (blue arrow).
On T2-weighted images tumour may be seen extending to or beyond the outer margin of the uterus. On contrast-enhanced imaging there is loss of the normal enhancing rim of myometrium.
In the 1998 FIGO staging for endometrial carcinoma,
peritoneal cytology was included in Stage IIIA disease. Although cytology is not included in the 2009 staging criteria,
it must still be reported as an additional feature.
Stage IIIB: Vaginal and/or parametrial involvement
On T2-weighted imaging there is focal loss of the normal low signal intensity of the vaginal wall indicating involvement (Figure 12).
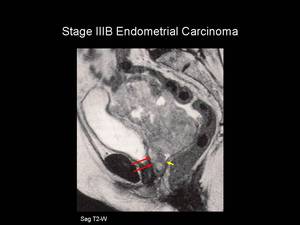
Fig.: Figure 12. Stage IIIB Endometrial Carcinoma. Sagittal T2-weighted image in a post-menopausal female. The entire uterus is replaced with intermediate T2-weighted signal intensity material which is seen to extend inferiorly to involve the anterior vaginal wall (red arrow). The posterior vaginal wall returns normal low T2-weighted signal intensity (yellow arrow).
References: Dr S Liyanage, Department of Radiology, Southend University Hospital
Stage IIIC: Metastases to pelvic and / or para-aortic lymph nodes
Stage IIIC1: Positive pelvic nodes (Figure 13)
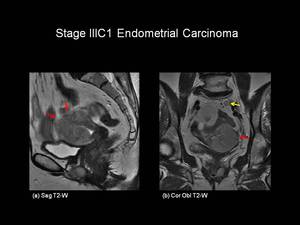
Fig.: Figure 13: Stage IIIC1 Endometrial Carcinoma. Sagittal (a) and coronal-oblique (b)T2-weighted images in a post-menopausal female. There is intermediate signal intenisty tumour extending from the endometrial cavity and replacing the myometrium. The serosal surface has been breached (red arrows). There is a left sided common iliac lymph node (yellow arrow), which has similar signal intensity to tumour - suggestive of lymph node involvement.
Stage IIIC2: Positive para-aortic lymph nodes with or without positive pelvic lymph nodes
Enlarged lymph nodes are low signal within high signal fat on T1-weighted images and intermediate signal intensity on T2-weighted images. Confusion between vessels and lymph nodes can be avoided since vessels contain flow voids (18).
Assessment of nodal involvement on standard MRI sequences mainly employs size based criteria (e.g.
>10mm in short axis diameter) as in computed tomography. However,
this does not always correlate with histological findings due to the high frequency of micrometastatic spread. Therefore these standard sequences are not optimal for detecting Stage IIIC disease and can only really be used for guidance of possible lymph node involvement (19),
with a reported sensitivity of only 50% and specificity of 95% in one study (20). Other techniques include using Ultrasmall particles of iron oxide (USPIO,
lymph node specific MRI contrast agent).
These have recently been shown to increase the sensitivity to lymph node metastases from 29 % to 93% but the future availability of these agents is now in question (21). 18F-FDG PET/CT has also shown to be of some use for detecting nodal metastases and may have an important role in the future.
Stage IV: Tumour invades bladder and/or bowel mucosa,
and/or distant metastases
On T2-weighted imaging,
the bladder or rectum wall are of low signal intensity,
interruption of this signal is indicative of tumour invasion. For true FIGO stage IV classification,
tumour should be visible within the bladder or rectal lumen at cystoscopy or colonoscopy respectively. MRI is able to suggest earlier invasion before tumour invades through the entire wall of these adjacent organs.
Stage IVA: Tumour invasion of bladder and / or bowel mucosa (Figure 14).
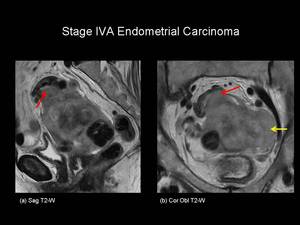
Fig.: Figure 14. Stage IVA Endometrial Carcinoma. Sagittal (a) and coronal oblique (b) T2-weighted images through the pelvis of a post-menopausal female. Intermediate signal intensity tumour is seen to replace the normal uterine tissue with serosal breach. In addition tumour extends to involve the sigmoid colon (red arrows) and the pelvic side wall (yellow arrow). Upper abdominal imaging also revealed hydronephrosis.
References: Dr S Liyanage, Department of Radiology, Southend University Hospital
Stage IVB: Distant metastases,
including intra-abdominal metastases and / or inguinal lymph nodes.
Delayed dynamic contrast-enhanced imaging is best for peritoneal deposit detection,
however the accuracy of detection reduces if deposits are less than 10mm (5).

 to the long axis of the endometrial cavity (solid red line). These sequences can then be used for accurate assessment of myometrial invasion by tumour. If there is suspected cervical invasion, further imaging is recommended on a plane perpendicular to the long axis of the endocervical canal.")

 and axial oblique T2-weighted (b) images in a post-menopausal female. On the T2-weighted images the endometrial cavity is distended with intermedaite signal intensity tumour (red arrows). The tumour has invaded the anterior myometrium by less than 50% (yellow arrows).")
. Imaging has been obtained from the same patient used in Figure 3. The uterine cavity is distended with high signal intensity material on the low b-value series which remains of high signal intensity on the high b-value series (red arrows). On the corresponding Apparent Diffusion Coefficient (ADC) map the lesion is of low signal intensity (yellow arrow) in keeping with tumour. This was histologically confirmed to represent grade 2 endometrial adenocarcinoma.")
 and coronal oblique (b) T2-weighted images in a post-menopausal female. Intermediate signal intensity tumour is seen distending the endometrial cavity with loss of the normal low signal intensity junctional zone. The tumour is seen to extend through greater than 50% of the myometrium (red arrows), but does not breach the uterine serosa.")
 and sagittal T1-weighted fat suppressed post-gadolinium (b) images in a post menopausal female. On the T2-weighted image, the endometrium is distended with intermediate signal intensity of tumour (red arrow). There is suspicion of deep myometrial involvement, however the post-contrast images demonstrate that there is actually less than 50% myometrial invasion (yellow arrows) making this Stage IA endometrial carcinoma. Confirmed histopathologically following hysterectomy.")
 demonstrates low signal intensity on T2-weighted imaging and can be seen to distort the normal zonal anatomy of the uterus. It is difficult to assess the degree of myometrial invasion by the intermediate signal intensity of the tumour (T).")
 T2-weighted and T1-weighted (b) fat suppressed post- gadolinium images in a post menopausal female. There is intermediate signal intensity tumour seen distending the endometrial cavity (red arrows). The juntional zone is widened with evidence of adenomyosis (yellow arrows) making evalution of myometrial invasion difficult. This tumour was Stage IA on histopathology.")
 and coronal-oblique (b) T2-weighted images in a post-menopausal female. There is a large intermediate signal intensity tumour (T) expanding the endometrial cavity. The tumour disrupts the normal low signal intensity of the junctional zone at the uterine fundus (red arrow) but does not involve greater than 50% of the myomterum indicating Stage IA disease. Myometrial thinning makes assessment of depth of invasion difficult.")
 and sagittal T1-weighted post gadolinium (b) in a post-menopausal female. There is intermediate T2-W signal intensity tumour filling and expanding the endometrial cavity (red arrows). In addition the tumour is seen to extend into the anterior lip of the cervix (yellow arrow). Note: tumour is seen to enhance less than the avidly enhancing myometrium.")
 and axial post-contrast T1-weighted fat saturated images through the pelvis in a postmenopausal female. The endometrial cavity is expanded by intermediate T2-W signal intensity material which shows enhancement following gadolinium administration (red arrows). In addition there is an enhancing metastatic nodule seen on the right ovary (yellow arrows) and a peritoneal deposit seen posterior to the urinary bladder (blue arrow).")
. The posterior vaginal wall returns normal low T2-weighted signal intensity (yellow arrow). References: Dr S Liyanage, Department of Radiology, Southend University Hospital")
 and coronal-oblique (b)T2-weighted images in a post-menopausal female. There is intermediate signal intenisty tumour extending from the endometrial cavity and replacing the myometrium. The serosal surface has been breached (red arrows). There is a left sided common iliac lymph node (yellow arrow), which has similar signal intensity to tumour - suggestive of lymph node involvement.")
 and coronal oblique (b) T2-weighted images through the pelvis of a post-menopausal female. Intermediate signal intensity tumour is seen to replace the normal uterine tissue with serosal breach. In addition tumour extends to involve the sigmoid colon (red arrows) and the pelvic side wall (yellow arrow). Upper abdominal imaging also revealed hydronephrosis. References: Dr S Liyanage, Department of Radiology, Southend University Hospital")