Type:
Educational Exhibit
Keywords:
MR, Bones, Neuroradiology spine, Musculoskeletal bone, Musculoskeletal spine, CT, Infection
Authors:
J. Kavanagh, R. Dunne, J. Keane, A. M. Mc Laughlin; Dublin/IE
DOI:
10.1594/ecr2011/C-1917
Imaging findings OR Procedure details
Plain Film,
CT and MRI all have roles in diagnostic imaging of TB Spondylitis.
Plain Film
Non specific plain film abnormalities such as osteopenia and soft tissue swelling can point the Radiologist towards the right diagnosis in the appropriate clinical setting.
Examples below Demonstrate bony abnormalities from the cervical spine down to the lumbar spine in our patient cohort.
In all cases plain film was the first investigation performed.
 Fig.: Increase in Atlanto-Axial distance and Paravertebral soft tissue swelling  Fig.: Loss of Right Pedicle of T5 |
 Fig.: Gibbous Deformity with Collapse |
|
CT vs MRI
CT is superior to MRI in the evaluation of the degree of bony destruction,
deformity and calcification.
The degree of destruction of the vertebra is seen much more clearly in the second example below on CT compared to MRI.
CT can be very useful in a paraspinal "cold abscess".
Calcification within this can virtually diagnose TB infection as well as indentify a small area of lytic bone disease.
 Fig.: Collapse of T11/T12 with retropulstion of bone fragments posteriorly |
 Fig.: T2 Weighted MRI showing T11/T12 involvement and spinal cord compression |
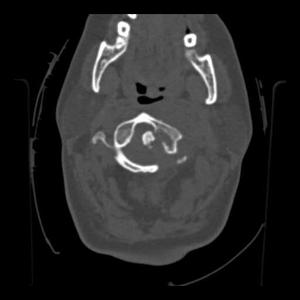 Fig.: Axial Bone windows demonstrating degree of bony destruction C1 |
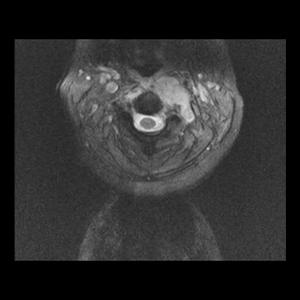 Fig.: Axial T2 weighted image showing extension through foramen transversarium and paraspinal abscess |
MRI
MRI is the Gold standard of imaging in TB Spondylitis due to its superior soft tissue resolution and multiplanar capability.
The Classic pattern of spread starting anteriorly and moving to involve opposing vertebrae via subligamentous spread is clearly seen on MRI.
The most common findings on MRI are decreased signal intensity on T1 weighted images and increased signal intensity on T2.
Paraspinal abscesses and disk herniation threatening the spinal cord can diagnosed accurately and quickly treated.
In contrast to pyogenic infections such as S.
Aureus,
TB generally spares the intravertebral disc due to the absence of proteolytic enzymes.
In rare cases when the disc is involved there will be increased signal intensity on T2 weighted imaging.
There is minimal periosteal reaction and sclerosis with TB and the anterior vertebral elements are preferentially involved,
which can be useful in differentiating it from metastatic disease.
In general,
however,
TB Spondylitis has many mimics such as fungal infection and sarcoidosis,
the clinical picture and obtaining tissue samples being vital in accurate diagnosis.
 Fig.: T1 Sagittal Pre Contrast Image  Fig.: T1 Post Contrast image with enhancing soft tissue mass extending through the posterior endplate into the intrathecal space displacing the spinal cord  Fig.: Saggital T2 weighted image |
 Fig.: T1 Para-Sagittal Pre Contrast  Fig.: T1 post contrast para-saggital image showing TB extending laterally into right paraspinal space 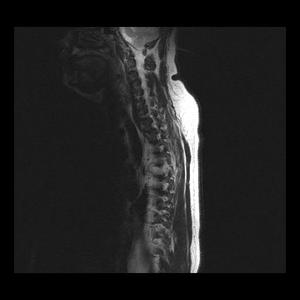 Fig.: Parasaggital T2 showing paraspinal abscess |
MRI
