Type:
Educational Exhibit
Keywords:
Osteoporosis, Metastases, Imaging sequences, MR, Neuroradiology spine, Musculoskeletal spine
Authors:
H. T. Koay, R. Dutta, M. George; Singapore/SG
DOI:
10.1594/ecr2012/C-0444
Imaging findings OR Procedure details
- Chemical shift imaging applies principle that fat and water protons in a single voxel show slightly different precession frequencies.
- Using a 1.5-T magnet,
water and fat protons are in phase with one another at a TE of 4.6 milliseconds.
At a TE of 2.4 milliseconds,
water and fat are 180° opposed; thus,
the signals of water and fat cancel each other.

Fig. 1: Physical principles of in-phase/opposed-phase imaging
References: AJNR June 2006 27: 1183-1188
- In normal bone marrow with the presence of both fat and water,
signal loss will occur on the out-of-phase images as compared with the in-phase images.
- Most malignancy completely replaces or displaces fat in the marrow space and will lack normal signal dropout on opposed phase images.
- While most benign conditions such as trauma,
edema,
marrow hyperplasia,
ischemia and infection do not replace bone marrow fat and preserve some degree of signal dropout on opposed phase images.
- In one of the study of 30 patients,
relative SI ratio to predict whether lesions were neoplastic or non neoplastic,
was calculated.
A 0.81 was used as cutoff value,
sensitivity and specificity of 95% were achieved.
This technique has also been used to differentiate acute benign versus malignant vertebral fractures.
(Disler DG,
McCauley TR,
Ratner LM,
Kesack CD,
Cooper JA.
In-phase and out-of-phase MR imaging of bone marrow: prediction of neoplasia based on the detection of coexistent fat and water.
AJR 1997; 169:1439–1447)
 Fig. 7: T1W
References: TTSH, Singapore |
 Fig. 8: T2W
References: TTSH, Singapore |
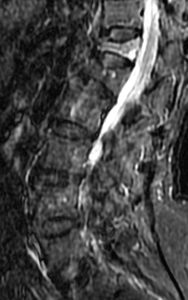 Fig. 9: FSEIR
References: TTSH, Singapore |
|
 Fig. 16: In-phase
References: TTSH, Singapore |
 Fig. 17: Opposed-phase: signal dropout
References: TTSH, Singapore |
Benign fracture of T12 and L1 vertebra with known metastatic colon carcinoma
 Fig. 10: T1W
References: TTSH, Singapore |
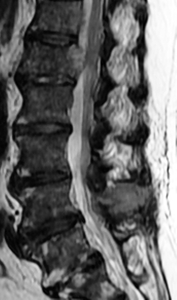 Fig. 11: T2W
References: TTSH, Singapore |
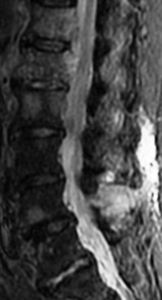 Fig. 12: FSEIR
References: TTSH, Singapore |
 Fig. 13: T1W + contrast
References: TTSH, Singapore |
 Fig. 18: In-phase
References: TTSH, Singapore |
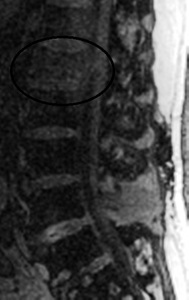 Fig. 19: Opposed-phase: no signal dropout
References: TTSH, Singapore |
Malignant fracture of L1 vertebra with known metastatic lung carcinoma
- There are several pitfalls in chemical shift imaging.
Radiation therapy may normalize the signal-to-noise ratio in treated lesions,
whereas marrow fibrosis may result in a false-positive interpretation.
Susceptibility artifact associated with sclerotic metastases and fracture-related hematoma may result in a false-positive result.
On the other hand,
metastases containing fat such as renal cell carcinoma and infiltrative multiple myeloma,
may result in a false-negative interpretation.
(Lubdha M.
Shah,
Christopher J.
Hanrahan.
MRI of spinal bone marrow: part 1,
techniques and normal age-related appearances.
AJR 2011; 197:1298–1308)
- Diffusion-weighted imaging (DWI) is a special technique using very strong magnetic gradients,
effectively canceling signal from protons in free moving water.
- All benign vertebral compression fractures were hypo- to isointense to adjacent normal vertebral bodies.
Pathologic compression fractures were hyperintense to normal vertebral bodies.
(Baur A,
Stäbler,
Brüning R,
et al.
Diffusion weighted MR imaging of bone marrow: differentiation of benign versus pathologic compression fractures.
Radiology 1998; 207:349–356)
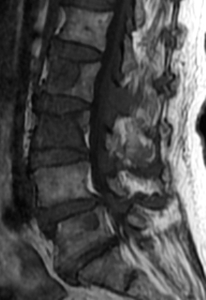 Fig. 4: T1W
References: TTSH, Singapore
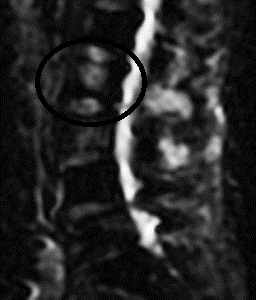 Fig. 23: DWI: restricted diffusion
References: TTSH, Singapore |
 Fig. 5: T2W
References: TTSH, Singapore
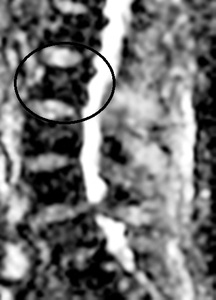 Fig. 22: ADC: low value
References: TTSH, Singapore |
| |
|
Expansile bony metastasis at L2 vertebra with known metastatic renal cell carcinoma
- Quantitative diffusion imaging with ADC (apparent diffusion coefficiency) mapping improved the distinction between benign and malignant lesions.
- It is known that ADC is sensitive to cell volume fraction and cellularity in biologic tissue.
- In metastatic lesions,
the cellularity can be high,
especially in actively growing tumors.
The lower ADC values in the metastases with high cellularity are seen.
- On the other hand,
the cellularity in benign fractures can be lower than that of metastatic lesions and leads to a higher ADC value.
-
The mean ADC value of benign lesions was 68% higher than that of the metastases.
(Xiaohong Joe Zhoua, Norman E.
Leedsa, Graeme C.
McKinnonb, Ashok J.
Kumara. Characterization of Benign and Metastatic Vertebral Compression Fractures with Quantitative Diffusion MR Imaging. AJNR 2002 23: 165-170)
 Fig. 2: T1W
References: TTSH, Singapore |
 Fig. 3: T2W
References: TTSH, Singapore |
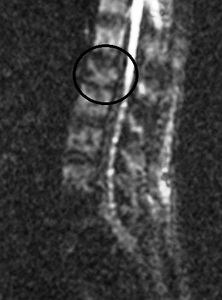 Fig. 20: DWI: no restricted diffusion
References: TTSH, Singapore |
 Fig. 21: ADC: high value
References: TTSH, Singapore |
Acute benign compression fracture of L1 vertebral body with known metastatic cervical carcinoma
