CASE 1
A 6-year-old autistic boy,
who suffered from cerebral palsy and underwent a Percutaneous Endoscopic Gastrostomy (PEG) tube for feeding since long time,
was complaining of recurrent chronic vomiting.
Abdominal X-ray was obtained (Fig 1),
presenting hyper lucent right upper quadrant by the presence of bowel air while the hepatic shadow was seen in the midline.

Fig. 1: Fig.1: Supine abdominal plain film shows the opacity of the liver deviated to the left side with the positioning of the right colon angle immediately under the right diaphragm.
Followed real time abdominal Ultrasonography (Fig 2) confirmed the mobility of the liver which was moving in a transverse axis to the midline in left lateral decubitus position of the patient and then to its normal anatomical position in the right hypochondrium when positioning the patient in right lateral decubitus.
The gallbladder was noticed initially to be midline then right paramedian with the movement of the patient as well as the liver hilum.
Large bowel loops were interposed in the right sub-diaphragmatic region.
There were no abnormalities of the hepatic and portal veins.
No signs of swirling of neither the hepatic hilum nor the mesenteric root were indentified.
The inferior vena cava maintained its normal position.
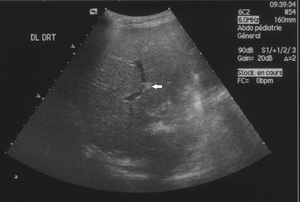
Fig. 2

Fig. 3: Fig.2: Ultrasound images demonstrate the mobility of the liver while shifting from right (a) to left (b) lateral decubitus. Note the direction of the bifurcation of portal veins (arrow).
An upper GI barium series demonstrated a normal position of the gastro-oesophageal junction without reflux.
The duodenum and ligament of Treitz were in orthotopic position as well.
The patient benefited from laparoscopic hepatopexy to prevent further hepatic mobility that might complicate the situation.
Per-operatively (Fig 3),
the surgeon found that the triangular suspensory ligament was very lax with elongated and mobile round ligament.

Fig. 4
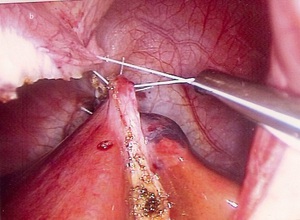
Fig. 5: Fig.3: (a) & (b) Laparoscopic fixation of the liver.
CASE 2
A 13-year-old boy presented to the emergency department with chronic intermittent vague and dull abdominal pain associated with vomiting.
His past surgical history included repaired inguinal hernia and orchidopexy.
His blood work up was normal with no leukocytosis.
Hepatic function test was normal.
Abdominal plain film was also unremarkable.
Abdominal ultrasonography was done,
and "incidentally" showed a mobile liver in the transverse plane while manipulating the patient (Fig 4).
In left lateral decubitus position,
the liver moves towards the left side and passes the midline.
The inferior vena cava in its retro hepatic segment seems tethered.
No signs of swirling neither of the portal vein nor of the mesentery root are present.
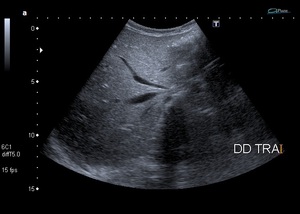
Fig. 6
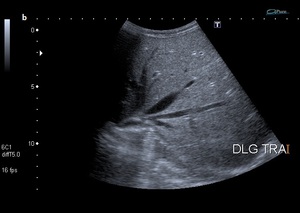
Fig. 7
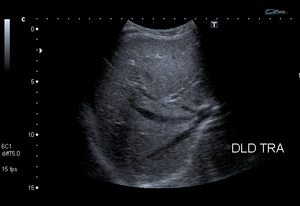
Fig. 8
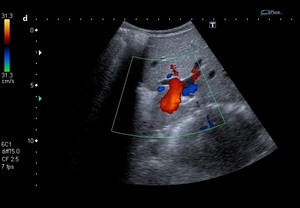
Fig. 9: Fig.4: Dynamic abdominal ultrasound reveals the mobility of the liver while manipulating the patient.
a)Dorsal decubitus. b) Left lateral decubitus. c) Right lateral decubitus. d) Color Doppler image shows hepatic pedicle directing into the left side.
To strengthen this exceptional diagnosis,
a Magnetic Resonance Imaging of the abdomen with dynamic maneuvers was performed (Fig 5) and confirmed the diagnosis of non-complicated hyper-mobile liver.
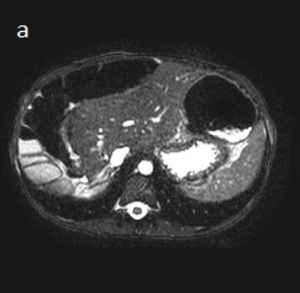
Fig. 10
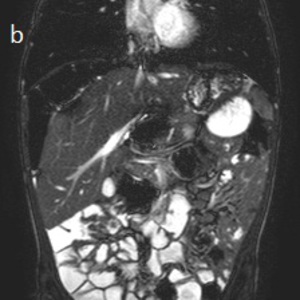
Fig. 11: Fig.5: (a) Axial and (b) coronal MRI TRUFISP images show the midline position of the liver with interposition of multiple loops of right colon between the diaphragm and the liver.
A cine-MRI sequence was performed and reinforced the real-time US findings (video available,
supplemental material in Sidebar).
Five months later,
another Magnetic Resonance Imaging (Fig 6) was done to reevaluate the status of the mesocolon before taking the decision for a preventive laparoscopic hepatopexy.
It demonstrated a harmonious distension of colon and with no transition zone that could suggest associated Hirschprung disease.

Fig. 12
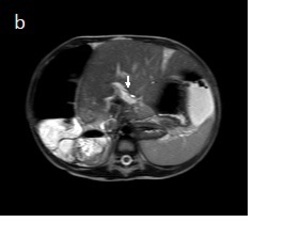
Fig. 13: Fig.6: A: Coronal MR SSH weighted-image shows the displacement of the gallbladder to the left side of the abdomen. B: Axial MR SSH weighted-image demonstrates displacement of the liver to the left upper quadrant and stretching of the hepatic pedicle (arrow).
Note; the harmonious distension of the colon is best seen on the coronal plane.
Laparoscopic hepatopexy was decided.
Per-operatively (Fig 7),
they noticed hyper mobile liver with redundant mesocolon.
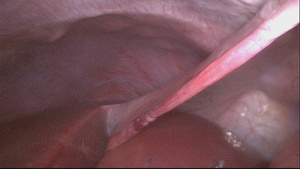
Fig. 14
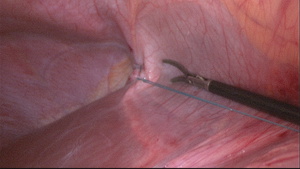
Fig. 15: Fig.7: An elongated round ligament seen during laparoscopic fixation of the liver.
DISCUSSION:
Hepar ambulens,
hepatoptosis,
hepatic ectopia,
hepatocolonic vagrancy and wandering liver are terms referring to the hepatic hypermobility,
as a consequence of lack of normal hepatic fixation that leads to displacement of the liver in the transverse plane around the inferior vena cava and changing its normal position according to the dependent side.
The wandering liver is a rare entity especially among the pediatric population.
The majority of cases,
in general,
are acquired-type.
There are reports of congenital-type cases.
The early diagnosis of such clinical condition is considered a challenge in the medical practice unless it is associated with colonic volvulus or hepatic pedicle torsion.
The liver is normally located in the right upper quadrant of the abdomen,
immediately inferior to the diaphragm.
It is suspended by the inferior vena cava and hepatic veins as well as by the hepatic suspensor apparatus including the triangular,
coronary and falciform ligaments.
The hepato-diaphragmatic connective tissue contained within the bare area and the muscular tone of the abdominal wall play a role as well.
Any congenital,
developmental or acquired anomaly of these factors may lead to abnormalities of hepatic fixation (hyperlaxity or absence of the suspensory ligaments) permitting an excessive mobility of the liver.
Embryologically,
the mesentery divides into ventral and dorsal segments.
The ventral mesentery develops into the suspensory ligaments and into the lesser omentum,
while the dorsal mesentery gives rise to the mesocolon.
Although there is no proved hypothesis explaining the relation between the hepatic hypermobility and colonic volvulus,
some authors thought that this embryological fact might explain it in case of persisting ventral mesentery interrupting the migration of the liver to the right (1,
8).
In contrast,
we noticed among the reported cases,
as well in our second case,
the “coincidence” of the wandering liver and the presence of redundant mesocolon.
The clinical presentation of wandering liver is variable and non-specific.
The hypermobile liver is often an asymptomatic condition and diagnosed incidentally or during the investigation of bowel obstruction.
It could be presented simply as unexplained chronic intermittent,
bizarre abdominal pain or as recurrent vomiting (9).
Furthermore,
Grayson et al described a case of unexplained sinus tachycardia that had been diagnosed with wandering liver and he mentioned that the wandering liver could be included in the differential diagnosis of sinus tachycardia (5).
Reviewing the literature,
we found the majority of the previously reported cases presenting with complication of excessive mobility of the liver in the form of hepatic torsion,
or with complication of an associated mesocolon redundancy leading to colonic volvulus.
Tate et al described in 1993 a patient presenting with hypotension and abdominal distension who was operated on.
Per-operatively,
they found colonic volvulus with hepatic torsion.
When the liver is displaced inferiorly ( hepatoptosis ),
a part of bowel loops,
frequently the large bowel, might be interposed in the right upper quadrant between the right diaphragm and the upper border of the liver,
which is called Chilaiditi’s syndrome.
The diagnosis in our cases was made regarding the presence of chronic abdominal pain and vomiting.
Nevertheless,
one can reasonably infer that the nutritional intolerance or the PEG tube feeding could explain the recurrent vomiting as we had seen with our first patient.
As all symptoms are rather non specific,
the early diagnosis of wandering liver is considered difficult,
but it is essential to prevent the complications in the future and consequently to consider a preventive selective hepatopexy (8).
Therefore,
most of cases are diagnosed incidentally in adulthood,
either per-operatively in case of surgical emergency complication or during the investigation of bowel obstruction.
Among the pediatric patients,
the diagnosis might be established by an abdominal plain film,
abdominal ultrasound or upper gastrointestinal series as working up the diagnosis of malrotation (11).
The computed tomography (CT) scan and the magnetic resonance imaging (MRI) with multiplanar reformations play a role in strengthening and reinforcing the diagnosis and in searching for associated anomalies (1,
3,
8,
and 12).
Our cases demonstrate:
- The usefulness of dynamic manoeuvres with ultrasound when the standard scan is normal and the abdominal pain is atypical.
- The usefulness of dynamic manoeuvres with MRI to reinforce the diagnosis suspected with US and to help the surgeon to decide for preventive surgery.
