ECR 2012 / C-0724
Spontaneous perforation of the colon: CT findings and clinical characteristics
Congress:
ECR 2012
Poster Number:
C-0724
Type:
Scientific Exhibit
Keywords:
Statistics, Decision analysis, Computer Applications-General, CT, Emergency, Abdomen, Colon, Inflammation, Obstruction / Occlusion
Authors:
H. Cho1, H. Y. Han1, T. J. Chun2, I. K. Yu1; 1Daejon/KR, 2Daejeon/KR
DOI:
10.1594/ecr2012/C-0724

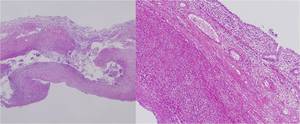
1B. Ascending colonic wall thining, acute and chronic inflammatory infiltrates with fibrinoid vasculitis, and ischemic change in the whole layer of the ascending colon wall (HE, x 100)")
Fig. 1:
1A. Perforation of the bowel wall (HE, x 40)
1B. Ascending colonic wall...
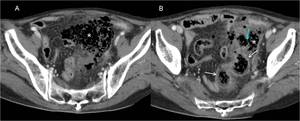
 shows large amount of fecal spillage(*) from distal sigmoid colon and continuous sigmoid colonic wall (arrow).
2B. There is sigmoid colonic wall defect (blue arrow) on the next coronal CT scan image.")
Fig. 2:
2A. 70-year-old woman with spontaneous sigmoid colon perforation. Coronal image...
.
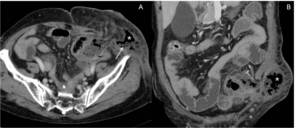
3B. On the 2.5 cm inferior from Figure 3A, there is focal sigmoid colonic wall defect (blue arrow) and fecal spillage from the defect site(*). There is diffuse edematous colonic wall thickening of sigmoid colon as a secondary sign of peritonitis(white arrows).")
Fig. 3:
3A. Abdominal CT shows large amount of fecal spillage in pelvic cavity(*)....
 and fecal spillage(arrow) from perforation site of colostomy.")
Fig. 4:
71-year-old woman with spontaneous colostomy site perforation.
Contrast...
 and colonic wall thickening(arrow).
There is extraluminal free air(*) as specific finding of colonic perforation.")
Fig. 5:
72-year-old woman with spontaneous descending colon perforation.
On axial...
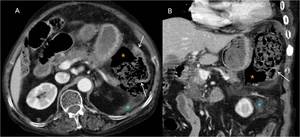
due to constipation.
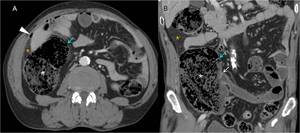
On axial image and coronal image of CT show fat infiltration(*), much dilatation of ascending colon up to 9 cm without any obstruction of colon. Some part of colonic wall is very thin(blue arrow). White arrow indicates ileocecal valve which is intact. Terminal ileum is normal.
There is extraluminal free air(arrowhead) as specific finding of colonic perforation.")
Fig. 6:
74-year-old man with spontaneous ascending colon perforation with severe fecal...
and air-fluid level without much dilatation of small bowel (arrow).
7B. Contrast enhanced CT shows peritoneal thickening with enhancement(arrows) as the sign of secondary peritonitis.
There is linear transverse colonic wall defect(red arrow) with free air just next to colonic wall defect.")
Fig. 7:
7A. 50-year-old man with transverse colon perforation.
Plain abdomen erect...