Craniosynostosis is the premature fusion of cranial sutures,
which results in deformity of the skull and may be accompanied by neurological impairment.
This diagram shows the different sutures which can be involved.
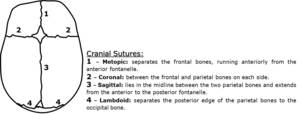
Fig. 1: Diagram of a neonate`s skull depicting location of major cranial sutures.
The birth incidence of craniosynostosis ranges from 3 to 6 per 10,000 live births [1,2].
In global perspective,
there is really no meaningful differentiation between males and females although coronal synostosis is more frequently seen in girls while sagittal synostosis is more common in boys [3,4].
Simple craniosynostosis is a term applied when only one suture is involved whereas complex or compound craniosynostosis is used to describe premature fusion of multiple sutures.
The primary or nonsyndromic variety constitutes 70-85% of cases and with descending frequency involve the sagittal suture, followed by coronal,
metopic and lambdoid [3] - table 1.
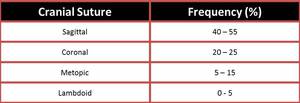
Table 1: Table 1 – Frequencies of isolated synostosis.
However about 15% to 30% may present as part of a craniofacial syndrome.
There are at least 180 such known causes and the most common syndromes are Crouzon, Apert,
Carpenter,
Chotzen and Pfeiffer.
Multiple theories have been proposed for the etiology of craniosynostosis,
but the most currently accepted defend one of several genetic mutations as the critical starting point.The mutations that have been described,
in syndromal and nonsyndromal forms,
include the fibroblast growth factor receptor-1 (FGFR1),
FGFR2,
FGFR3 and the transcripton factor genes TWIST1 and MSX2 [5].
However,
secondary craniosynostosis may result from a known underlying condition,
such as metabolic (hyperthyroidism,
renal osteodystrophy,
hypercalcemia,
hypophosphatasia),
hematologic disease (polycythemia vera,
sickle cell disease,
sickle cell anemia and talassemia),
drugs or mechanical causes [3,5,6].
In normal conditions,
calvarial bones grow perpendicular to suture lines but premature fusion averts it.
This is balanced by increased growth parallel to the direction of the affected suture and additionally with progressive widening of normal adjacent sutures.
The nature of the subsequent skull deformity depends on which sutures are involved and the time of onset.
Imaging plays a key role because the clinical presentation is variable and early diagnosis is essential for proper management and prevention of complications.
Intracranial pressure (ICP) may be elevated in isolated (55% increased risk) or multiple synostosis that increases risk by 90%,
including signs as papilledema,
vomiting,
and lethargy.
Furthermore,
aesthetic deformity,
mental retardation,
seizures and other neurological impairments have also been stated.
