Five patients were male; ages ranged between 35 and 65 years.
The lesions had saccular morphology and 15mm in diameter or larger,
only one demonstrated intra-renal location.
The procedures were performed in an average of 53 (range 19-92) minutes.
Patient 1 suffered the spontaneous rupture of a previously asymptomatic aneurysm.
The aneurysm was located in a bifurcation of the main anterior branch,
and we decided to perform the embolization of the lesion and the segmental branch arising from it.
In this case was necessary to perform two procedures to achieve the proper embolization.
In the first procedure we made an attempt to embolize the aneurism using coils.
Nevertheless,
the device escaped from the lesion and to cover the neck of the aneurysm,
was necessary to implant two overlapped stent grafts (Fig.
2).
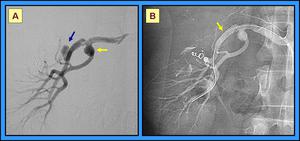
Fig. 2: A. Angiography shows a saccular aneurysm in a bifurcation of the main anterior branch (blue arrow) and a fusiform aneurysm in the main posterior branch (yellow arrow). B. After implantation of two 5mm stent grafts (yellow arrow), both the aneurysm as the segmental artery arising from it, showed proper exclusion. Due to the location of the fusiform aneurysm, next to the bifurcation of the main renal artery, we decided not to perform any endovascular treatment.
Seven months later,
on a control CT we observed reperfusion of the aneurysm.
Angiography demonstrated the filling of the lesion through a leakage between the stent graft and the inner edge of the artery (Fig.
3).
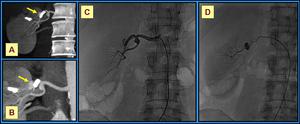
Fig. 3: A-C. Coronal MIP image and angiography showing reperfusion of the aneurysm (yellow arrow) and the segmental artery. D. Through a 5 Fr hydrophilic coating Cobra catheter, a 2.7 Fr micro-catheter was inserted between the intima and the stent graft. The leakage is clearly demonstrated.
We placed a 2.7 Fr catheter between the intima and the stent graft to infuse micro-particles for end-artery embolization.
Then two micro-coils were implanted to seal the leakage completely (Fig.
4).
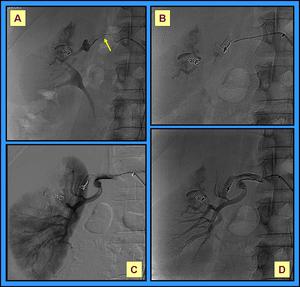
Fig. 4: A. Procedure of end-artery embolization by infusion of micro-particles (500 micrometers), that were stained with contrast agent, through the micro-catheter (yellow arrow). B-D. After implantation of the micro-coils, angiography shows the proper seal of the leakage and a segmentary infarct affecting the renal upper pole.
Patient 2 suffered severe abdominal traumatism which provoked fracture of the right inferior renal pole.
Angiography clearly showed the renal lesion and a pseudo-aneurysm in a segmental branch.
To avoid surgery and excision of the kidney,
we elected a conservative endovascular procedure consisting in the embolization of the inferior renal artery with coils and implantation of a 5mm stent graft covering the neck of the pseudo-aneurysm.
In this procedure we were able to exclude properly the pseudo-aneurysm and to embolize the inferior renal pole (Fig.5).

Fig. 5: A and B. Angiography of the right kidney demonstrating renal fracture and a pseudo-aneurysm. C. Final control angiogram demonstrating coil embolization of the inferior pole artery (red arrow). Moreover, the stent graft (blue arrow) has excluded the pseudo-aneurysm.
Patient 3 and patient 5 were treated with similar procedures.
Both patients showed small neck saccular aneurysms.
The aneurysms were treated by means of insertion of fibered micro-coils with controlled detachment through a 2.5 Fr micro-catheter; the procedures allowed the near complete exclusion of the lesions (Fig.
6 and Fig 7).
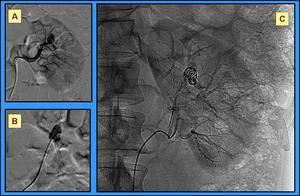
Fig. 6: Patient 3.A. Angiography showing the saccular aneurysm. B and C. Through a micro-catheter placed inside the aneurysm we inserted two fibered micro-coils with controlled detachment, of 20 and 10mm in length.
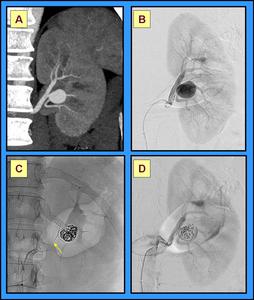
Fig. 7: Patient 5. A and B. Coronal MIP multi-slice CT image and angiography showing the aneurysm. C and D. Through a micro-catheter placed inside the aneurysm eight fibered micro-coils with controlled detachment were inserted. In this case a 0.018-guidewire (yellow arrow) was placed to prevent coil migration.
Patient 4 suffered from hypertension,
and on CT scan presented a wide neck saccular aneurysm in the main posterior branch,
next to the bifurcation of the right renal artery.
To diminish the diameter of the neck,
we placed a stent for covering the aneurysm (Fig.
8).
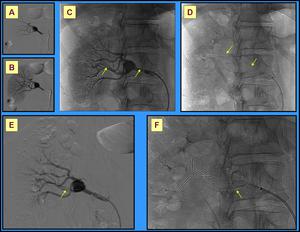
Fig. 8: A and B. Angiography of the right kidney showing a wide neck saccular aneurysm. C and D. Through a 6 Fr introducer sheath, two 0.014 guidewires were placed in the main arterial branches (yellow arrows). E and F. One 5mm balloon-mounted stent was placed covering the aneurism.
Then,
a 2.5 Fr micro-catheter was inserted in the aneurismal sac,
where three fibered micro-coils with controlled detachment and two conventional micro-coils of variable dimensions were rolled up (fig.
9).
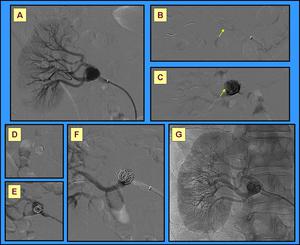
Fig. 9: A-F. Through a micro-catheter placed in the aneurysm (yellow arrow) five micro-coils were inserted. G. Post-coiling control angiogram revealed complete aneurysm exclusion with integrity of renal vasculature.
Patient 6 had renal transplantation.
Next to the anastomosis between the left outer iliac artery and the renal artery of the graft,
a pseudo-aneurysm was found (Fig 10).
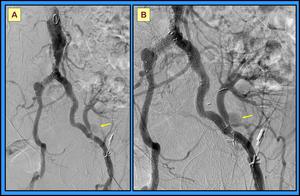
Fig. 10: A. Aortoiliac angiography to evaluate the vasculature of the renal graft. B. Pseudo-aneurysm in the main artery of the graft (yellow arrow).
A 5 Fr hydrophilic coating Cobra catheter was placed inside the sac of the pseudo-aneurysm,
to insert conventional coils and to achieve the embolization of the lesion (Fig.
11).
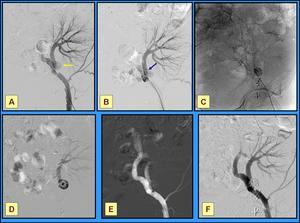
Fig. 11: A. Selective iliac angiography, pseudo-aneurysm (yellow arrow). B and C. 5 Fr hydrophilic coating Cobra catheter (blue arrow) inside the pseudo-aneurysm. D and E. Five conventional coils were placed into the lesion. F. Post-coiling control angiogram revealed complete aneurysm exclusion with integrity of graft vasculature.
Follow up. Patients were followed by periodic multi-slice CT,
for an average of 31 (range 12-42) months.
All patients were successfully treated,
and in successive multi-slice CT we did not found other complications (Fig 12).
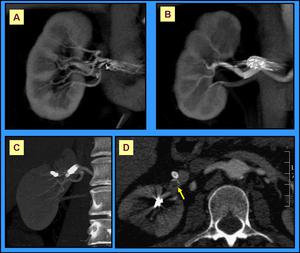
Fig. 12: A and B. Patient 4. Coronal 3D “volume rendering” one month after embolization procedure. Proper exclusion of the aneurysm. C and D. Patient 1. MIP multi-slice CT. 38 months after procedure, CT scan clearly demonstrates the trombosed aneurysm (yellow arrow).
