From May 2009 to November 2012 we performed seven consecutive endovascular therapeutic procedures,
in six patients affected by aneurysms (n:4) or pseudo-aneurysms (n:2) of the renal arteries.
Treatments were made to achieve the embolization of the lesions in patients with a high risk of rupture of the aneurysms and pseudo-aneurysms,
and to avoid a life threatening bleeding and/or nephrectomy.
One patient was asymptomatic and the lesion was detected on a CT scan performed by other circumstances without relation with renal pathology.
In three cases the lesions were detected in patients in arterial hypertension study.
One patient had suffered the spontaneous rupture of a previously asymptomatic aneurysm,
and other patient suffered an abdominal traumatism that provoked the rupture of the right kidney.
Lesions were evaluated on a 32-row scanner.
On multi-slice CT before treatment,
we studied location,
relationship with the arterial branches and size of the neck of the aneurysms and the pseudo-aneurysms (Fig.1); these data would be useful for planning the endovascular therapy.
Patient characteristics and morphological evaluation of the lesions are summarized in table 1.
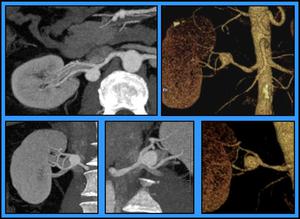
Fig. 1: Evaluating the morphology of the aneurysm by CT, Patient 4. Using MIP and 3D “volume rendering” we are able to depict the proper location of the lesion in the different arterial branches, and evaluate its morphology, size and diameter of the neck. This patient showed a wide neck (6mm) saccular aneurism, 17mm size, in the origin of the main posterior renal branch.
Therapeutic procedures were performed under local anesthesia and sedation,
and we used the right femoral approach in six cases and the left approach in one patient.
After femoral puncture,
a 5 or 6 French (Fr) introducer sheath,
was implanted intra-arterially,
next to the main renal artery on the side that was to be treated.
Then,
a 5 Fr Renal or Cobra braided catheter was placed inside the main renal artery to perform an angiographic study.
According with size,
location and characteristics of the neck,
we used different endovascular techniques,
single or combined: embolization by conventional coils or fibered micro-coils with controlled detachment,
stenting,
stent-graft exclusion and end-artery embolization with micro-particles.
The length of the whole procedure,
from the time of femoral approach to angiography for testing the embolization,
was also considered.
For monitoring the success of the procedures,
periodic multi-slice CT were carried out to all patients.
In general,
scans were performed one month and six months after treatment; later,
patients underwent annual image studies.
Therapeutic procedures on each case are summarized in table 2,
in one patient was necessary to perform two consecutive embolization procedures.


