ECR 2013 / C-0882
Imaging and pathologic findings of congenital intracranial tumors in fetus and infant: A pictorial review
Congress:
ECR 2013
Poster Number:
C-0882
Type:
Educational Exhibit
Keywords:
Foetus, Congenital, Diagnostic procedure, Contrast agent-intravenous, Ultrasound, MR, CT, Paediatric, Neuroradiology brain, CNS
Authors:
I. Popescu, V. M. Marcu, M. C. Coman, S. Tarnoveanu, C. Cirstoveanu, S. Stoica ; Bucharest/RO
DOI:
10.1594/ecr2013/C-0882

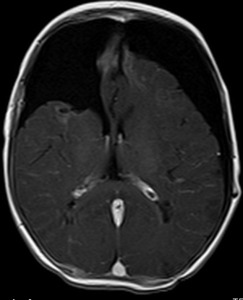
Fig. 1:
B, 10w. Axial T2-weighted MR image shows marked hypointensity and flow voids...

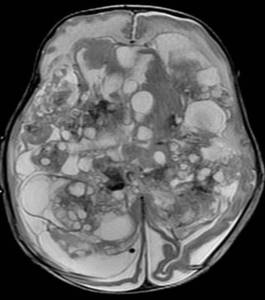
Fig. 2:
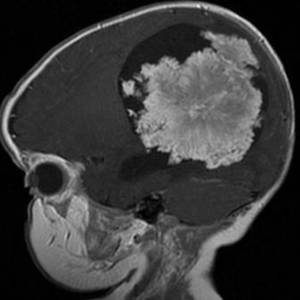
B, 10w. Contrast-enhanced sagittal T1-weighted MR image shows a large,...

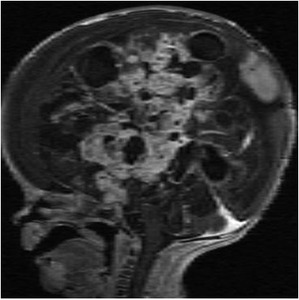
Fig. 3:
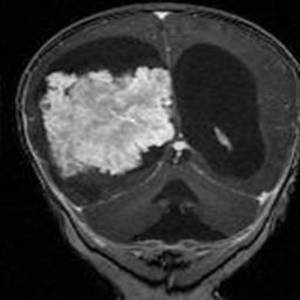
B, 10w. Contrast-enhanced coronal T1-
weighted MR image shows intense...

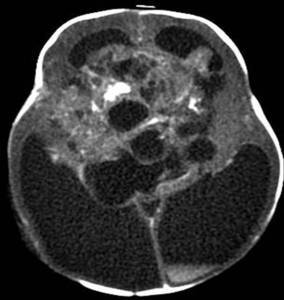
Fig. 4:
B, 4y, Follow-up MDCT, coronal MPR shows right-sided residual hygroma and...
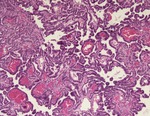
Fig. 22:
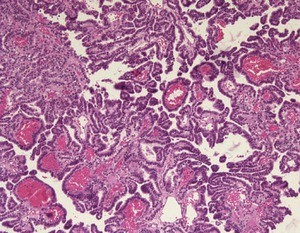
Choroid plexus papilloma. Photomicrograph
(original magnification, 40;...

Fig. 5:
V, 7d. Clinical appearance of cutaneous hemangiomatosis.

Fig. 6:
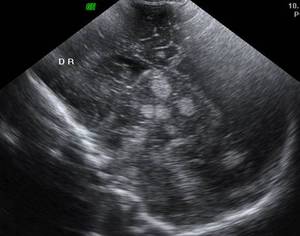
V, 7d. Convex probe - sagittal view US reveals multiple hyperechoic nodular...

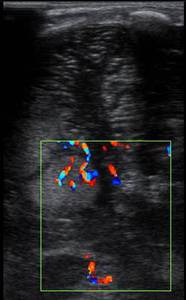
Fig. 7:
V, 7d. Liniar probe - trans mastoid view shows Color Doppler signal within the...

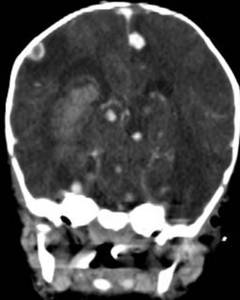
Fig. 8:
V, 7d. Follow-up coronal MPR MDCT at 1 month shows progressive disease: the...

Fig. 9:
V, 7d. Sagittal MPR contrast-enhanced MDCT at 1 month shows increased...

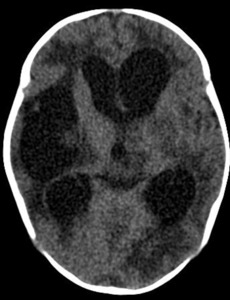
Fig. 10:
V, 7d. Follow-up MDCT at 4 months shows porencephalic cavities, posthemorrhagic...

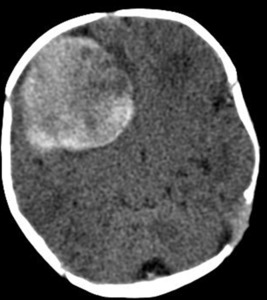
Fig. 11:
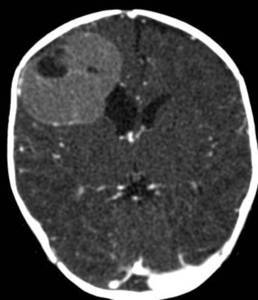
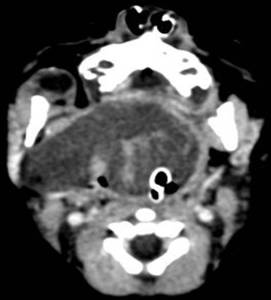
A, 13d. MDCT shows a spontaneous hyperdense right frontal lesion, that was...

Fig. 12:
A, 13d. 1 month follow-up contrast-enhanced axial MDCT shows the low,...

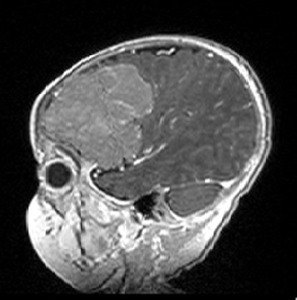
Fig. 13:
A, 13d. Contrast-enhanced sagittal T1 weighted shows lobulated, slightly...

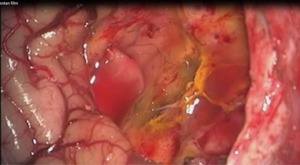
Fig. 14:
A, 13d. Surgical exposure of the tumor.

Fig. 15:
A, 13d. 4 months postoperative axial T1 weighted contrast enhanced MRI shows no...

Fig. 16:
A, 7d. Contrast enhanced axial MDCT shows cystic and solid, heterogeneous...

Fig. 17:
A, 7d. Contrast-enhanced T1 weighted shows cystic and solid, heterogeneous...

Fig. 18:
A, 7d. Follow-up at 6w axial T2 weighted MRI shows rapidly growth of the...

Fig. 19:
R, preterm, 1d. Contrast enhanced axial MDCT shows an inhomogeneous enhancing...

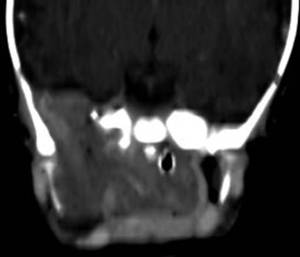
Fig. 20:
R, preterm, 1d. Coronal contrast enhanced reformated MDCT shows the tumor...

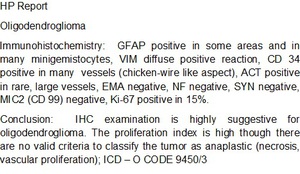
Fig. 21:
A, 13d. HP report.