PORTAL SYSTEMIC COLLATERAL VESSELS:
Portosystemic collateral vessels develop in patients with portal hypertension as a way to decompress the splachnic flow,
and they can be divided into two groups depending on whether they drain toward the superior vena cava (SVC) or the inferior vena cava (IVC).
- Collateral vessels draining into the SVC include the left gastric vein (coronary),
short gastric vein,
posterior gastric vein,
gastric varices,
esophageal and paraesophageal varices.
- Vessels draining into the IVC include gastrorenal and splenorenal shunts,
paraumbilical vein and abdominal wall veins,
retroperitoneal and mesenteric shunts,
mesenteric varices,
gallbladder varices and omental collateral vessels.
Portosystemic shunts can be classified in intrahepatic or extrahepatic.
Although the intrahepatic shunts have been the most common documented,
the extrahepatic ones also have an important role,
and can be also subdivided depending on their relation with superior mesenteric vein (SMV) or,
less frequent,
with inferior mesenteric vein (IMV).
Inferior mesenteric vein shunts (IMVS) connect IMV to inferior vena cava (IVC),
and are an exceedingly rare type of shunt with few cases reported in the literature.
They have a tortuous appearance,
and have been described mainly in portal hypertension clinical situations or secondary to postsurgical fascia adhesions,
although some of them are considered to be congenital.
Until recently it was thought that formation of collateral circulation was due to the passive opening of vascular channels in response to increased portal pressure.
However,
some recent studies have shown that in splanchnic neovascularization may also be involved proangiogenic molecules like vascular endothelial growth factor (VEGF) or platelet-derived growth factor (PDGF).
EMBRIOLOGY:
In the fifth week of intrauterine life,
there are three major paired veins in the abdomen: the vitelline (or also called onphalomesenteric),
the umbilical and the cardinal veins.
The vitelline veins form the hepatic sinusoids.
The left vitelline vein subsequently involutes and the blood is diverted into the right vitelline vein,
which enlarges and forms the hepatocardiac portion of the inferior vena cava (IVC).
Derivatives of the vitelline veins also form the hepatic and portal vein (Table 1).
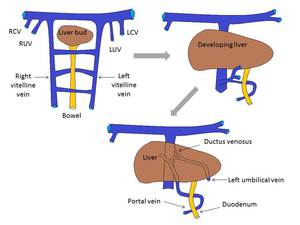
Table 1: Development of the hepatic venous system.
Vitelline veins form the hepatic sinusoids. Left umbilical vein connects to the right vitelline vein via the ductus venosus. Anastomotic network around the duodenum forms the portal vein.
LCV: left cardinal vein; RCV: right cardinal vein; RUV: right umbilical vein; LUV: left umbilical vein.
References: Maria Pardo
The cardinal venous system consists of the anterior,
posterior,
and common cardinal veins.
Afterwards,
between fifth and seventh weeks,
the cardinal venous system is formed additionally with supracardinal,
subcardinal and sacrocardinal veins.
The IVC is formed between the sixth and eighth gestational weeks sequentially by the formation,
anastomoses and posterior regression of three paired embryonic veins: the posterior cardinal,
the subcardinal,
and the supracardinal veins (Table 2).
It is composed of four segments: infrarenal,
renal,
suprarenal,
and hepatic segments.
The subcardinal system gives rise to the prerenal segment of the IVC.
The anastomosis between subcardinal and supracardinal systems forms the renal vein segment.
The supracardinal system gives rise to the postrenal segment of the IVC.
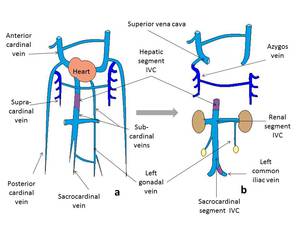
Table 2: Development of the cardinal venous system from weeks 5-7 to birth.
a) At 5-7 weeks.
b) At term.
References: Maria Pardo
Aberrations in the complex embryogenesis of the IVC recently mentioned above result in several potential anatomic variants,
present in approximately 4% of the population.
IMV ANATOMY:
On cross sectional imaging,
the IMV is visualized running in the left paraduodenal space and forming an arc cephalad to the duodenojejunal junction before its termination.
Its major tributaries are the superior hemorrhoidal vein,
the sigmoid vein and the left colic vein.
Usually the IMV terminates into the splenic vein,
but anatomical variations can include the IMV draining into the splenoportal angle and the IMV draining into the SMV.
Extrahepatic portosystemic venous shunts are caused by persistent communication between the vitelline vein and subcardinal veins,
resulting in abnormal confluence of the portal vein and the inferior vena cava tributaries.
Since Retzius reported on,
several anastomoses between the portal venous system and the IVC in the retroperitoneum,
anastomoses between branches of the SMV or IMV and the IVC have generally been called the veins of Retzius.
These retroperitoneal pathways between the tributaries of the mesenteric vein and vena cava are considered a remnant of fetal communication,
and it is often difficult to completely trace the drainage course due to the complex and often extensive nature of these collateral vessels that appear as small,
rounded or tubular areas of increased attenuation that enhance to the same degree as the mesenteric veins.
A similar prevalence of veins of Retzius has been described in patients with and without portal hypertension.
Portal systemic encephalopathy in patients without liver cirrhosis or portal hypertension has also been described,
although it is extremely rare.
