Practical Analysis
Let’s play a game! Imagine…
- On a day like any other day,
we are in the US examination room when the emergency department consults us about a baby with suspected infantile hypertrophic stenosis of the pylorus.
Do you know the characteristics of a child with suspected infantile hypertrophic stenosis of the pylorus?
Patients with suspected infantile hypertrophic stenosis of the pylorus are usually between two and eight weeks old,
although this condition has been reported in babies as young as one week and as old as five months.
These babies tend to lose weight despite a large appetite.
Typically,
they develop nonbilous vomiting after meals,
with blood-stained vomit due to gastritis,
that increases to become “projectile”.
If diagnosis and treatment are delayed,
hypertrophic stenosis of the pylorus can lead to dehydration,
hypochloremic alkalosis,
sodium and potassium deficiency,
and paroxysmal aciduria.
Is it considered an immediate radiologic emergency?
No,
it is considered a relative radiologic emergency.
The first and most important thing is to stabilize the patient and correct any electrolyte disturbances.
Surgery should be deferred until the infant is appropriately resuscitated.
What do you think is the best imaging technique to establish the diagnosis?
For more than 20 years,
high resolution US has been the first choice for diagnosing infantile hypertrophic stenosis of the pylorus: it is noninvasive,
fast,
widely available,
economical,
does not require contrast agents,
does not use ionizing radiation,
and has nearly 100% sensitivity and specificity.
High resolution US enables the direct visualization of the muscle and of the pyloric canal.
Nowadays,
barium upper gastrointestinal series are reserved for patients in whom the US findings are inconclusive and those in whom reflux is strongly suspected.
The clinical diagnosis hinges on palpation of the thickened pylorus or “olive”.
Abdominal palpation is accurate but not always successful,
depending on factors such as the experience of the examiner,
the presence of gastric distention,
and a calm infant.
How should the US be done? Should the stomach be full or empty?
High-resolution linear probes (7-15 MHz) should be used.
These probes are capable of identifying all the layers of the pylorus.
The stomach should not be emptied before the examination because this makes identification of the antropyloric area difficult.
If the stomach is filled with gas,
placement of the patient in a right anterior oblique position permits fluid to gravitate to the antrum for adequate evaluation.
On the other hand,
if the stomach is markedly distended,
the duodenal cap may be displaced caudally and medially,
rendering the pylorus extremely difficult to access.
In such cases,
if the patient is slowly moved toward the supine and even the left posterior oblique position,
the pylorus will be able to rise anteriorly for optimal examination.
Less experienced practitioners should try to locate the gallbladder first.
The pylorus is usually located adjacent to the gallbladder (see axial and longitudinal diagrams).
Do you know the US appearance of a normal pylorus?
Although there is no general consensus about the normal measurements of the pyloric canal,
the most accepted figures are:
- Thickness of the muscle ≤3 mm,
and it is hypoechoic
- Anteroposterior pyloric diameter ≤ 14mm
- Length of the pyloric canal ≤ 17 mm
A good way for radiologists to remember these parameters is the mnemonic: P < 3.1416 (3 mm muscle thickness,
14 mm AP diameter,
and 16 or 17 mm long).
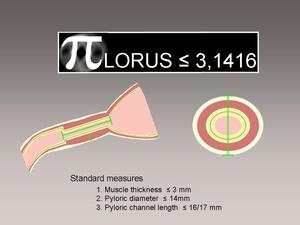
Fig. 2: Normal measures of the pyloric channel
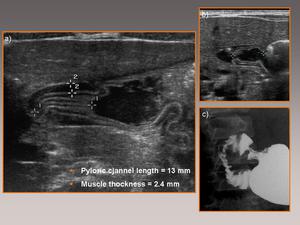
Fig. 3: Longitudinal slice from an abdominal sonogram showing the characteristics of the normal pylorus (a) with correct relations to the sphincter; note the passage of gastric contents through the sphincter (b). Note the correlation with the upper gastrointestinal tract examination (UGI).
Do you know the characteristic findings of infantile hypertrophic stenosis of the pylorus on US?
In hypertrophic stenosis of the pylorus,
thickening of the pyloric muscle leads to lengthening of the pyloric canal.
On US,
the hypertrophy of the pyloric muscle is seen as a heterogeneous hypoechoic ring with a hyperechoic center on transversal slices.
The hypoechoic ring corresponds to the thickened muscle and the hyperechoic center corresponds to the redundant edematous surface of the mucosa.
In longitudinal slices,
lengthening of the pyloric canal is seen as a characteristic image: the “double-track sign” (Fig.
9).
Additionally,
the pylorus bends and raises the duodenal bulb,
giving rise to the “umbrella sign”.
Both these signs correlate well with the images on barium upper gastrointestinal series.The presence of prolapsed pyloric cannel mucosa into the gastric antrum results in “the antral nipple sign".
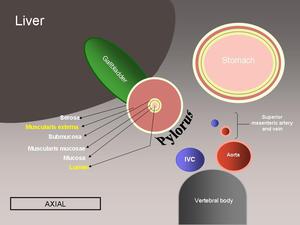
Fig. 4: Axial diagram showing the anatomic relations of a hypertrophic pyloric stenosis.
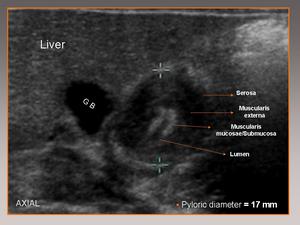
Fig. 5: Axial view showing the characteristic sonographic findings for hypertrophic pyloric stenosis.
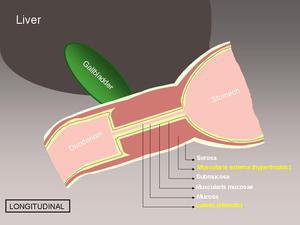
Fig. 6: Longitudinal diagram showing the anatomic relations of a hypertrophic pyloric stenosis.
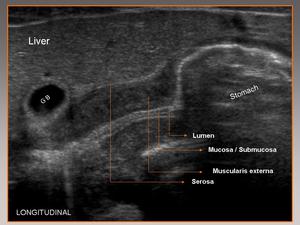
Fig. 7: Longitudinal view showing the characteristic sonographic findings for hypertrophic pyloric stenosis.
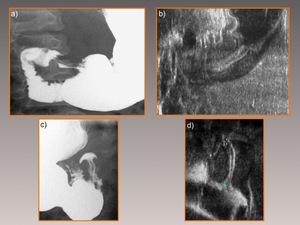
Fig. 8: Correlation between findings at sonography and UGI for the "double-track sign" (Figs. a & b) and for the "umbrella sign" (Figs. c & d).
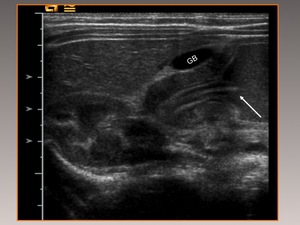
Fig. 9: Three-month-old patient with hypertrophic pyloric stenosis. Note the “nipple sign”: the presence of pyloric canal mucosa prolapsing into the gastric antrum (arrow).
A degree of hyperechogenicity may be seen in the hypertrophied pyloric muscle.
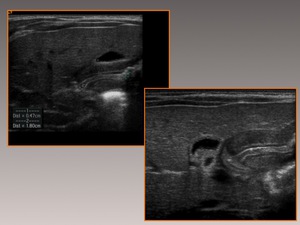
Fig. 10: One-month-old patient with a one-week history of nonbilous vomiting. Longitudinal slice shows marked thickening of the muscular layer of the pylorus. Note the slight hyperechogenicity.
Infantile hypertrophic stenosis of the pylorus causes exaggerated peristaltic waves in the gastric antrum,
a sign of the antrum struggling to overcome the pyloric stenosis.
In some cases,
it is possible to see the emptying of gastric contents and air into the duodenum through a hypertrophied pylorus (abdominal plain films can show proper intestinal pneumatization).
It is important to observe the failure of the pyloric canal to relax in real time!
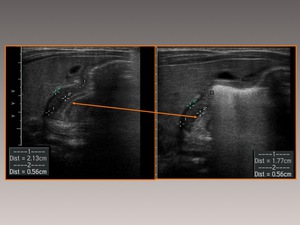
Fig. 11: Passage of gastric contents through a hypertrophied pylorus.
Can a child with normal findings on a US examination develop infantile hypertrophic stenosis of the pylorus?
Yes! The clinical syndrome always precedes the imaging findings; thus,
when US rules out infantile hypertrophic stenosis of the pylorus,
we should recommend clinical follow-up and repeating the US study within a few days.
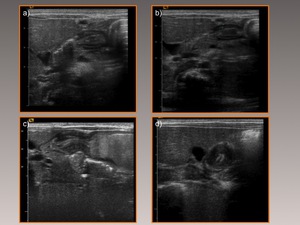
Fig. 12: Ten-day-old patient who presented with an episode of nonbilous vomiting. Sonogram shows a normal-appearing pylorus (Figs. a & b). Repeat sonogram 12 days later done for persistence of symptoms shows a clearly hypertrophic pylorus (Figs. c & d).
- Great! We have successfully diagnosed infantile hypertrophic stenosis of the pylorus! Now we need to contact the surgical team so they can operate on the child.
Do you know what the treatment consists of?
The current treatment of choice is pyloroplasty (Fredet-Weber-Ramsted extramucosal pyloromyotomy).
Before the operation,
electrolyte disturbances must be corrected.
Stabilizing the child can delay the intervention by 24 h to 48 h.
Like all surgical techniques,
complications can occur.
Medical treatment with antispasmodics (atropine) was used until the mid-1960s and is currently be reappraised by various investigators.
- After the intervention,
the child was discharged; however,
one week later he presented at the emergency department with persistent vomiting after meals.
What diagnostic possibilities should you consider?
If done correctly,
the surgical intervention solves the problem,
and no cases of relapse have been reported.
The characteristic US findings can persist for six to eight weeks after surgery,
which is the time necessary for the hypertrophied pyloric muscle to return to its normal size and appearance.
We should not consider these findings to represent failed surgery! In this case,
the cause of our patient’s vomiting was gastroenteritis.
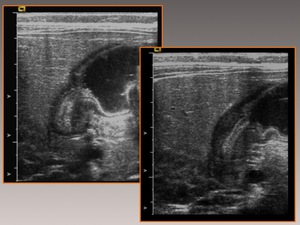
Fig. 13: Sonogram in a patient who presented a new episode of vomiting 15 days after intervention for hypertrophic pyloric stenosis shows that the hypertrophy of the pylorus persists.
