Definition and Etiology
Infantile hypertrophic pyloric stenosis,
the most common surgical condition producing emesis in infancy,
was first described by Hirschsprung in 1888.
The pyloric muscle is hypertrophied and the pyloric channel becomes narrow and elongated,
causing gastric outlet obstruction.
It typically develops between 2 and 8 weeks after birth.
The incidence is approximately 2 to 5 per 1000 live births.
It is more common in boys: the ratio of boys to girls affected is 4.8:1.
The cause is unknown,
although various genetic factors,
environmental factors (e.g.,
sleeping in the prone position,
erythromycin,
and maternal smoking,
among others),
and hormonal factors are thought to play a role in the pathogenesis.
It seems that various anomalies are present in the muscular layer,
including anomalous distribution of nerve endings,
peptide alterations,
decreased synthesis of nitric oxide (due to downregulation of the nNOS gene),
ultrastructural changes and decreased number of cells of Cajal,
and increased production of insulin-like growth factor.
Together,
these factors are thought to result in failure of the mechanism of muscular relaxation,
increasing the production of growth factors and giving rise to hypertrophy.
There is a familial predisposion.
Abaut 20% of the sons and 7% of daughters of female index cases develop the disease ,
whereas 5% of sons and 2% daughters of male index cases are affected.
Pylorus Anatomy
The pyloric portion is the most distal part of the stomach,
which is connected to the duodenum through the pyloric sphincter or ring.
The incisura angularis divides the stomach into the gastric body (to the right of this notch) and the pyloric part (to the left).
The pyloric part is further divided by the sulcus intermedius into two parts: the pyloric antrum (the most proximal part,
which connects to the body of the stomach) and the pyloric canal (the most distal part,
which connects to the duodenum).
The pyloric antrum terminates in the pyloric orifice,
in the pyloric sphincter.
The pyloric sphincter is a zone of intermittent high pressure.
It contains a circular layer of smooth muscle that is capable of both tonic and fascicular contraction,
enabling gastric emptying.
A definite separation between the pyloric sphincter and the gastric antrum or the head of the duodenum cannot be clearly identified.
Unlike most intestinal sphincters,
the pyloric sphincter maintains the same lumen (approximately 1 cm wide) most of the time.
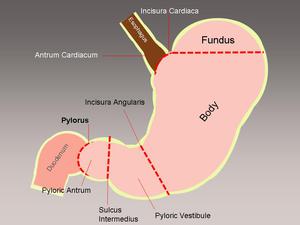
Fig. 1: Normal anatomy of the antro-pyloric region
