DTI parameters mean diffusivity,
MD and fractional anisotropy,
FA (which is the anisotropy normalized standard deviation of diffusion measurements in different directions) provide an exquisite and useful tool for non-invasive and intravoxel investigation of human tissue microstructures [15-17]
In this work,
we hypothesized that in cancellous bone,
bone marrow water is primarily restricted between bone trabeculae and bone marrow fat [13].
In such a situation water shows a slower dynamic compared to that of free water.
In particular,
since the amount of bone-marrow water compared to bone-marrow fat is higher in vertebrae than in the femoral neck,
water dynamic in the femoral neck is more restricted than in vertebrae.
As a consequence,
to optimize the measurements of water with a slower dynamic,
it is necessary to use higher b-values compared to those employed to perform DWI in vertebrae.
In this work,
selecting b=2500 s/mm2,
we measured an averaged MD approximately equal to 3*10-4 s/mm2 in the femoral neck.
This study shows significant differences in FA and MD indices in the femoral neck of postmenopausal women characterized by different BMD.
Because the results discussed here highlighted a strong correlation between FA and T-score,
they underline the greatest potential of a DTI rather than a DWI approach[18-22],
to assess osteoporosis disease in cancellous bone.
Unlike the contradictory results obtained in vertebral cancellous bone [18-21],
a clear relationship between MD and T-score was found in the femoral neck.
Data reported here show that MD depends on both FF and T-score and that FF results,
are well comparable to data from the literature [7,11].
Healthy data points displayed in Fig.
3a and 3b underline changes in MD mainly due to FF variations.
In pathological cases,
both FF and T-score vary.
Similarly,
healthy data points underline changes in FA mainly due to T-score variations,
while FA versus FF of healthy subjects are not characterized by a well defined trend.
In particular our data underlined that FA is characterized by a decreasing trend when moving from the healthy to the osteoporotic group. (fig.4)
Our results indicate that,
from a microscopic point of view,
with the development of osteoporosis,
the local anisotropy inside the cancellous bone pores decreases.
(fig.
4)
In this work,
we hypothesized that bone marrow water,
is more prevalent in the boundary zone while fat occupies primarily the central zone of the pore [18].
In the light of this assumption,
FA variations could be due to changes in the inner surface of pores (as an example associated with the roughness of the trabeculae surface or to the structure of the endosteum).
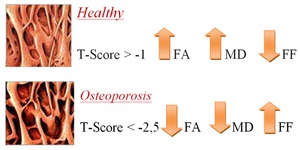
Fig. 4: Images of the microstructural findings in Healthy and Osteoporotic bone in correlation with the variations T-Score values, and the FA,MD and FF trends. In the osteoporitic bone FA an MD decrease end the Fat Fraction increase because of the loss of trabecular microstructure
We may hypothesize that with the development of the osteoporosis the environment probed by water restricted between fat and bone becomes more isotropic due to the structural rearrangement of the endosteum cell lines or of the trabeculae surface (FA results shown in this work are related to the variation of anisotropy that occurs at a length scale of approximately 10 µm).
On the other hand,
using a different length scale of the order of millimetres,
trabecular bone anisotropy increases with osteoporosis,
as well documented in literature [23,24].
Although the decreased FA values due to the increased loss of anisotropy in cancellous bone is the major effect when moving from healthy to osteoporotic status,
in this work we investigated FA/FF and MD/FF parameters to simultaneously exploit both the structural (MD and FA) and the metabolic (FF) variables for discriminating between healthy and pathological subjects
In this study,
the concordance between MD/FF,
FA/FF and DXA method is equal to 81.1% because osteopenic subjects are not well identified by MR parameters.
However,
osteopenia is not a well defined clinical pathology,
but it may be considered a transitional stage between normal and osteoporotic status.
Because DXA BMD evaluation is currently the gold standard for osteoporosis diagnosis,
the potential of the DTI-1H-MRS protocol for the evaluation of the osteoporosis in the femoral neck has been evaluated in relation to DXA results obtained in the same skeletal site.
Our data suggest that MD/FF together with FA/FF parameters may have potential as surrogate markers for the microarchitectural deterioration of cancellous bone.
In conclusion,
diffusion analyses with MD and FA parameters together with FF quantification,
make possible to obtain intravoxel information and novel details on the microstructure of cancellous tissue and the bone metabolism.
We have reported here the first DTI investigation of femoral
cancellous bone performed in three different BMD groups of postmenopausal women.
Although our results are still preliminary,
and based on a small number (N=37) of subjects,
they suggest the ability of MD/FF and FA/FF to discriminate between healthy and osteoporotic subjects.
In particular they indicate that DTI assessment in the femoral neck,
in combination with 1H-MRS investigations may be useful in the study of physiological changes associated with osteoporosis.
However,
further studies,
with a larger population,
are required to validate our preliminary findings.

