ECR 2013 / C-1266
Eardrum color and the imaging diagnosis of middle ear disease: otoscopic - radiologic correlation of retrotympanic lesions.
Congress:
ECR 2013
Poster Number:
C-1266
Type:
Educational Exhibit
Keywords:
Inflammation, Diagnostic procedure, MR, CT, Neuroradiology brain, Ear / Nose / Throat
Authors:
J. C. Tortajada Bustelo1, M. Prenafeta Moreno2, S. Perez Aguilera1, M. Cufí Quintana1, C. Spinu1, V. P. Beltrán Salazar1, A. Carvajal1, M. Zauner Jakubik1, A. Rovira Gols1; 1Sabadell/ES, 2Arenys de Munt-Barcelona/ES
DOI:
10.1594/ecr2013/C-1266

Fig. 1:
We classify the diseases according to the otoscopic findings into three major...

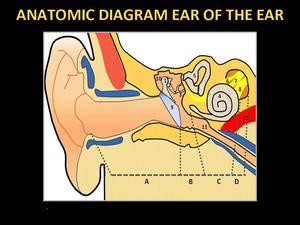
Fig. 2:
Anatomic diagram of the ear: 1. Malleus, 2. Incus, 3. Stapes, 4. Cochlea, 5....
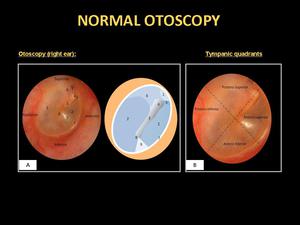
: 1. Flaccid portion, 2. Tense portion, 3. Manubrium, 4. Lateral process of the malleus, 5. Anterior fold of the malleus, 6. Posterior fold of the malleus, 7. Annulus, 8.Umbo, 9. Cone
of light.
B- Tympanic quadrants: The manubrium divides the eardrum into the anterior and posterior regions. If a line is also projected perpendicularly at the level of the umbo, the 4 classic quadrants are obtained: anterosuperior, posterosuperior, anteroinferior, & posteroinferior.")
Fig. 3:
A- Otoscopy (right ear): 1. Flaccid portion, 2. Tense portion, 3. Manubrium,...