Study design and case selection
The UK Lung Screen (UKLS) pilot trial is a randomised control trial that has been underway since 2011,
randomising 4000 subjects (2000 in each arm) aged between 50 and 75 years to either screening with LDCT or no screening [5].
Over a 20-week period between November 2011 and April 2012,
the LDCT studies of 290 consecutive participants in the LDCT arm of the UKLS were read prospectively for this study.
All LDCT scans were performed at two participating sites.
Classification of nodules
Nodules were classified according to UKLS categories as summarised in Table 1 [5].
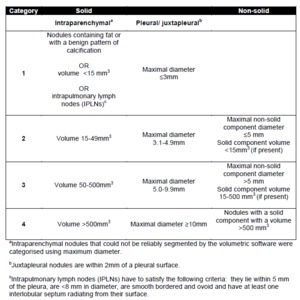
Table 1: UKLS categorisation of nodules.
A non-commercial database entry proforma (Artex VOF,
Logiton,
Netherlands) used for the UKLS study provided options for nodule categorisation,
slice and segment location.
LDCT reading by radiologists
Each LDCT scan was read by a single thoracic radiologist at each of the two participating sites (Radiologist A at Site 1 and Radiologist B at Site 2).
The scans were then transmitted to a central reading site for a second independent reading by Radiologist C.
A semi-automatic nodule segmentation package (Lungcare,
Siemens Medical Solutions,
Erlangen,
Germany) was used for volumetric analysis.
For pleural/ juxtapleural nodules or those with unreliable segmentation,
maximal diameter was measured instead.
Selection of reading radiographers
Four radiographers were selected as readers.
Radiographer 1 read scans at Local Site 1,
and Radiographer 2 read scans at Local Site 2.
Two radiographers (Radiographers 3 and 4) read scans at the central site.
As such,
each scan was read by two radiologists and between one and two radiographers (one local site radiographer and/or one central site radiographer).
All four radiographers had experience in thoracic CT scan acquisition,
and had been trained and tested on 100 LDCT scans as part of a training evaluation study,
using the same volumetric analysis software (Please see ECR 2013 Scientific Paper Control number 1964- "Feasibility of training radiographers to detect nodules in CT lung cancer screening").
Reference standard
Arbitration on discrepancies was provided at the central site by a thoracic radiologist with more than 20 years of experience,
and the final consensus view was recorded on the database.
All agreed category 2 to 4 nodules and intrapulmonary lymph nodes were considered positive in the reference standard.
Classification of discrepancies
For each LDCT study,
a list of the consensus nodules and each reader’s reading was generated.
A nodule was considered to have been omitted by a reader if it was included in the reference standard but not recorded by that reader.
Statistical analysis
The sensitivity (the percentage of consensus nodules identified) and the average false-positive detection (FP) rate per case were calculated:
- for each reader,
for all cases read by him or her;
- for each radiographer and radiologist within a particular radiographer-radiologist combination (10 combinations in total),
taking into account only cases read by that combination,
to enable direct comparison between that radiographer and radiologist (comparisons of sensitivity and average FP rates performed using McNemar’s test and paired student’s t-test,
respectively); and
- for each reader in the first 10 weeks (P1),
and compared to that in the second 10 weeks (P2) of the study (comparisons of sensitivity and average FP rates performed using the Chi-square test and independent samples student’s t-test,
respectively).
A p value of less than 0.05 was assumed to be statistically significant.
