Liposarcomas
Liposarcomas (LPS) are usually well-differentiated containing abnormal fat but with dedifferentiated components which appear more solid.
Other types such as myxoid,
pleomorphic and mixed type also occur but are less common.
Well Differentiated Liposarcomas (WDL) - have imaging characteristics similar to fat.
They tend to have nodular septations internal vascularity and a heterogenous texture.

Fig. 1: Well Differentiated Liposarcoma (WDL)- Large retroperitoneal mass predominantly of fatty attenutation with irregular nodular septations
References: Radiology Department, The Royal Marsden Hospital - London/UK
De-differentiated Liposarcomas (DDL) - usually have well defined solid components that are distinguishable from the fatty tissue.
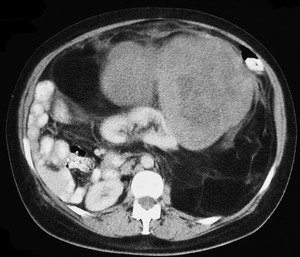
Fig. 2: Large De-differentiated Liposarcoma (DDL)- Note the septated, nodular fat density mass with a heterogenous enhancing soft tissue component.
References: Department of Radiology, Royal Marsden Hospital, London/UK
Leiomyosarcoma
Leiomyosarcoma's are the second most common primary RPS.
It is an uncommon malignant neoplasm of smooth muscle origin with a slight female predilection.
Imaging appearances are non-specific meaning that correct diagnosis requires immunohistochemistry.
Due to their indolent nature they can present late and of a significant size with the tumour undergoing necrotic or cystic changes centrally.
Calcification is a rare feature.
Occasionally venous extension into the IVC or retroperitoneal veins is noted.
These tumours demonstrate contrast enhancement peripherally if large.
Due to its superior soft tissue contrast resolution and multiplanar modality,
MRI also provides added value in retroperitoneal leiomyosarcomas [1,2].
It is useful in delineating the tumour's site of origin,
its margins and invasion of adjacent structures.
The signal intensity of the tumour is non-specific and variable depending on the degree of haemorrhagic and cystic changes,
but its imaging characteristics are as follows [2]:
T1 - isointense to muscle
T2 spin-echo - intermediate to hypointense to fat
T2 spin-echo fat saturation - predominantly hyperintense

Fig. 3: Leiomyosarcoma - Large enhancing soft tissue mass coming off the IVC and also invading into its medial wall. There is associated mass effect with displacement of adjacent structures.
References: Department of Radiology, Royal Marsden Hospital, London/UK
Malignant Fibrous Histiocytoma (MFH)
These generally appear as well circumscribed soft tissue density masses with some areas of lower attenuation.
They can range from hypervascular to hypovascular masses.
They have a tendency to arise from,
or be in close proximity to,
the kidneys and /or adrenal glands which may help in offering a differential with RPS [3].

Fig. 4: Malignant Fibrous Histiocytoma (MFH) - Soft tissue mass that appears to arise from the left kidney but closer inspection reveals a cleft fat plane between the left kidney and retroperitoneal mass lesion.
References: Department of Radiology, Royal Marsden Hospital, London/UK
Solitary Fibrous Tumour (SFT)
These are a rare group of spindle cell neoplasms that include fibrous to cellular solitary fibrous tumours (SFT)s and related lesions such as lipomatous haemangiopericytoma and giant cell angiofibroma.
They are most commonly located within the thorax although extra-thoracic locations include the retroperitoneum,
deep soft tissues of the proximal extremities,
abdominal cavity and head and neck.
SFT's tend to have a discrete lobulated contour,
are well defined and usually cause displacement of adjacent structures as opposed to invasion of adjacent structures.
Furthermore they are hypervascular demonstrating avid enhancement post contrast administration and often have large perilesion collateral feeding vessels [4].
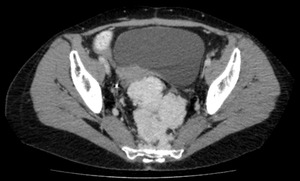
Fig. 5: Solitary Fibrous Tumour (SFT) - Lobulated mass, with a well defined contour causing displacement of adjacent structures and demonstrating avid enhancement post contrast administration.
References: Department of Radiology, Royal Marsden Hospital, London/UK
Chondrosarcoma
Extraskeletal chondrosarcomas are far less frequent than intraosseus chondrosarcomas and represent 2% of all soft tissue sarcomas. Histological subtypes of extraskeletal chondrosarcoma include myxoid (most common type),
mesenchymal and well-differentiated.
Classically they present as lobulated soft tissue masses with calcific foci.
Extensive calcification is more typical of extraskeletal mesenchymal chondrosarcoma than its skeletal counterpart,
whereas the myxoid variant has more amourphous and punctuate calcification.
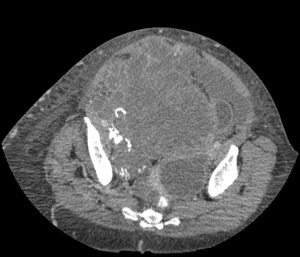
Fig. 6: Chondrosarcoma - Large lobulated soft tissue mass with calcific foci
References: Department of Radiology, Royal Marsden Hospital, London/UK
Ewing’s Sarcoma
Although commonly regarded as an osseous sarcoma in paediatric patients,
approximately 20% of Ewing's sarcoma family of tumours (ESFT) are seen in adults and are extra-skeletal in location.
ESFT represent a group of high-grade small round cell tumors,
including Ewing sarcoma of bone,
extra skeletal Ewing sarcoma,
peripheral primitive neuroectodermal tumor (PNET),
and Askin tumor (thoracopulmonary PNET).
These tumours can arise from solid organs and usually do not cross the midline.
ESFT has a propensity for the kidney and retroperitoneum and can invade adjacent organs or structures such as the vasculature (renal vein,
or inferior vena cava) similar to renal cell carcinoma [5].
In the retroperitoneum it can also invade the paraspinal regions with neuroforaminal and spinal invasion best assessed on MRI.
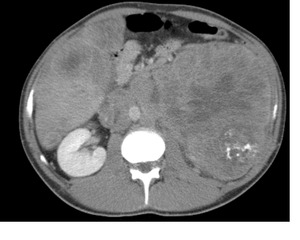
Fig. 7: Ewing Sarcoma Family of Tumours (ESFT) - Large retroperitoneal soft tissue mass originating from the kidney, not crossing the midline but demonstrating invasion of the adjacent vasculature. (NB the presence of liver metastases also).
References: Department of Radiology, Royal Marsden Hospital, London/UK
