During a period of five years (2006-2010),
we performed U/S examinations of the neck region in 285 patients (265 women; mean age,
43.2 years; range,
17–89 years) with known thyroid cancer,
looking for potential metastases before surgery as well as in postoperative follow-up,
without an already clinical known recurrent or residual thyroid cancer.
This was a retrospective study of 365 non palpable cervical lymph nodes detected sonographically and verified by real-time (Rt) ultrasonography-guided (Ug) fine-needle non-aspiration cytology (FNNAC) -Rt-Ug-FNNA(9).
Nodes were measured on the screen,
and their shape ( Fig. 1 ), cystic changes ( Fig. 2 ),
echogenicity ( Fig. 3 ),
microcalcifications ( Fig. 4 ),
vascularity ( Fig. 5 ), absence of hilus ( Fig. 6 ),
size,
and location were reported. Informed consent is the communication process between a patient and physician that results in the patient’s agreement to undergo a RtUg-FNNAC which was obtained (see Table 1).
| Table 1. The written informed consent form |
- The consent form was patient friendly and written so that the patient fully understands the procedure.
- The purpose of the biopsy was discussed with the patient.
- It was emphasized that a high percentage of cervical nodes are benign and that an adequate tissue sample with RtUg-FNNAC may eliminate the expense and potential morbidity of surgical excision with general anaesthesia.
- The RtUg-FNNAC procedure,
potential risks and complications were described.
- The possibility of a hematoma,
the most frequently occurring complication,
was mentioned.
- Notes were given in case of further complications.
|
For the U/S examination a high-resolution (7.5-15 MHz) linear-array transducer was used for real-time B-scans of the neck with a sterile cover placed over its head for Rt-Ug-FNNA.
After the target node had been localized on the preprocedural U/S examination,
the overlying skin was sterilized with chlohexidine gluconate.
Both sides of the neck were checked for the presence of enlarged lymph nodes.
All lymph nodes were scanned in the longitudinal plane,
and the largest diameter was measured (maximum diameter).
Nodes larger than 5 mm in maximum diameter were considered enlarged.
The lymph nodes were divided into levels according to their location: level I of the neck (the superior third of the neck including submental - region 1 and submandibular nodes - region 2),
level II (upper jugular nodes - region 3 and region 4),
level III (the mid third of the neck -middle jugular level nodes - region 5),
level IV (the inferior third of the neck -including low jugular nodes - region 6),
level V (the supraclavicular regions - region 7 and the posterior triangle - region 8) and level VI (midline low neck - central compartment nodes incorporate the Delphian/prelaryngeal,
pretracheal,
and paratracheal lymph nodes) (15,16) ( Fig. 7 ).
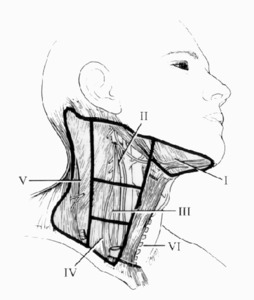
Fig. 7: The lymph node surgical regions of the neck are divided into levels I through VII: 1) level I nodes are the submental and submandibular nodes; 2) level II are the the upper jugular nodes; 3) level III are the midjugular nodes; 4) level IV are the lower jugular nodes; 5) level V are the supraclavicular nodes and posterior triangle; 6) level VI or central compartment nodes incorporate the Delphian/prelaryngeal, pretracheal, and paratracheal lymph nodes; and 7) level VII nodes are those within the superior mediastinum.
References: modified from Taylor S. (1975) Surgery of the thyroid gland. In DeGroot LJ, Stanbury JB: The Thyroid and its Diseases, 4th ed. New York, John Wiley & Sons: pp 776–779
We performed Rt-Ug-FNNA of the most suggestive nodes from the tumor drainage region in one or both sides of the neck.
In the case of a solitary node,
authors punctured it; in the case of multiple nodes,
authors chose 1,
2,
or more nodes,
depending on their sonographic appearance and position in the neck.
Rt-Ug-FNNA was performed by a freehand technique.
A plane perpendicular to the ultrasonographic probe for needle insertion was chosen.
The puncture was performed with a conventional 23 (or 25) gauge needle without an attached syringe,
for cell collection(9) ( Fig. 8 ).

Fig. 8: Freehand biopsy technique without aspiration: the needle is placed just above the transducer without an attached syringe (Rt-Ug-FNNAC). This nonaspirate technique relies on capillary action to draw the sheared cells within the small-caliber needle.
References: modified from Gkeli MG et al. (2011) Submandibular ectopic thyroid tissue diagnosed by ultrasound-guided fine needle biopsy. J Oral Sci 53: 249-252
The patient was placed in a supine position with the neck slightly extended and superimposed on a pillow for his/her convenience.
Instead of U/S gel,
a topical anaesthetic lidocaine/prilocaine jelly was used during the procedure as it served as a primary coupling agent.
The needle was inserted vertically into the target node,
centrally in the transverse U/S-image,
while the angle of the needle was on a nearly coaxial plane to the axis of transverse image.
The used angle was shallow (~600) for superficial nodes and steeper (<300) for deeper ones.
The needle tip was carefully monitored during the procedure.
Once the needle was entered into the node,
it was oscillated gently back and forth in various positions and directions without aspiration under real time U/S attendance for a few seconds only by movement of the operator's wrist ( Fig. 9 ).
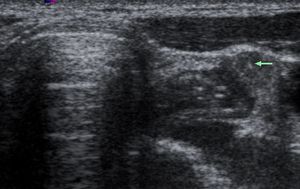
Fig. 9: Gray-scale sonogram of patient with unpalpable metastatic node. Image of 34-year-old woman with DTC and associated occult metastatic node in left central cervical region shows the needle tip (arrow) inside the node.
When a small amount of material filled the hub of the needle,
the needle was withdrawn and the puncture site on the skin was compressed for a few minutes.
This nonaspirate technique relies on capillary action to draw the sheared cells within the small-caliber needle.
Smears were stained by Quick Giemsa stain and Pap-method and the ultimate diagnoses were made by cytopathologists.
In the case of smears with inadequate material for reliable cytologic diagnosis (4.8%),
we repeated the Rt-Ug-FNNA to obtain adequate material.
Final diagnoses were determined by the histologic examination from excision biopsy when performed or by the clinical (monitoring of thyroglobulin –Tg- and antithyroglobulin antibody levels) and U/S follow-up for more than 12 months (to 36 months).
All cytologically verified malignant nodes were confirmed histologically after surgical removal.
When a lymph node diagnosed as benign by Rt-Ug-FNNAC was unchanged or regressed spontaneously on U/S follow up and there was not any detectable Tg,
the diagnosis made by the Rt-Ug-FNNAC was considered correct.
When a lymph node diagnosed as benign by Rt-Ug-FNNAC increased in size with subsequent management or became palpable at clinical follow up or there was detectable Tg without already clinical known recurrent or residual thyroid cancer,
excisional biopsy was performed.
Patients with clinical known recurrent or residual thyroid cancer were excluded from this study.
Diagnostic yield,
sensitivity,
specificity,
accuracy,
and complications of Rt-Ug-FNNAC were evaluated.







 level I nodes are the submental and submandibular nodes; 2) level II are the the upper jugular nodes; 3) level III are the midjugular nodes; 4) level IV are the lower jugular nodes; 5) level V are the supraclavicular nodes and posterior triangle; 6) level VI or central compartment nodes incorporate the Delphian/prelaryngeal, pretracheal, and paratracheal lymph nodes; and 7) level VII nodes are those within the superior mediastinum. References: modified from Taylor S. (1975) Surgery of the thyroid gland. In DeGroot LJ, Stanbury JB: The Thyroid and its Diseases, 4th ed. New York, John Wiley & Sons: pp 776–779")
. This nonaspirate technique relies on capillary action to draw the sheared cells within the small-caliber needle. References: modified from Gkeli MG et al. (2011) Submandibular ectopic thyroid tissue diagnosed by ultrasound-guided fine needle biopsy. J Oral Sci 53: 249-252")
 inside the node.")