ECR 2013 / C-1742
Diagnostic value of ultrasound-guided fine-needle aspiration cytology in diagnostics of solid renal lesions
Congress:
ECR 2013
Poster Number:
C-1742
Type:
Scientific Exhibit
Keywords:
Cancer, Efficacy studies, Biopsy, Ultrasound, Oncology, Kidney
Authors:
D. Plut, S. Ponorac, D. Vidmar-Bracika; Ljubljana/SI
DOI:
10.1594/ecr2013/C-1742

Fig. 2:
Curved array multifrequency transducer with a detachable biopsy guide.

Fig. 3:
21 gauge spinal needle used to perform aspiration biopsy.

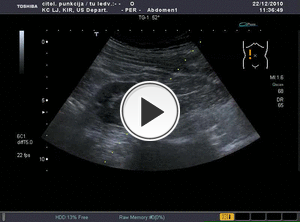
Fig. 4:
Localization of the solid renal lesion with a projected trajectory for the...

Fig. 6:
Insertion of the spinal needle. One radiologist inserts the needle through the...

Fig. 7:
Aspiration of material for cytologic review.

Fig. 8:
Nurse prepares aspirated material for the transportation to the cytologist.